























| 图片: | |
|---|---|
| 名称: | |
| 描述: | |
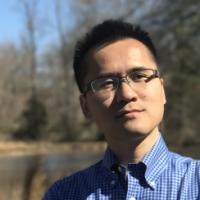
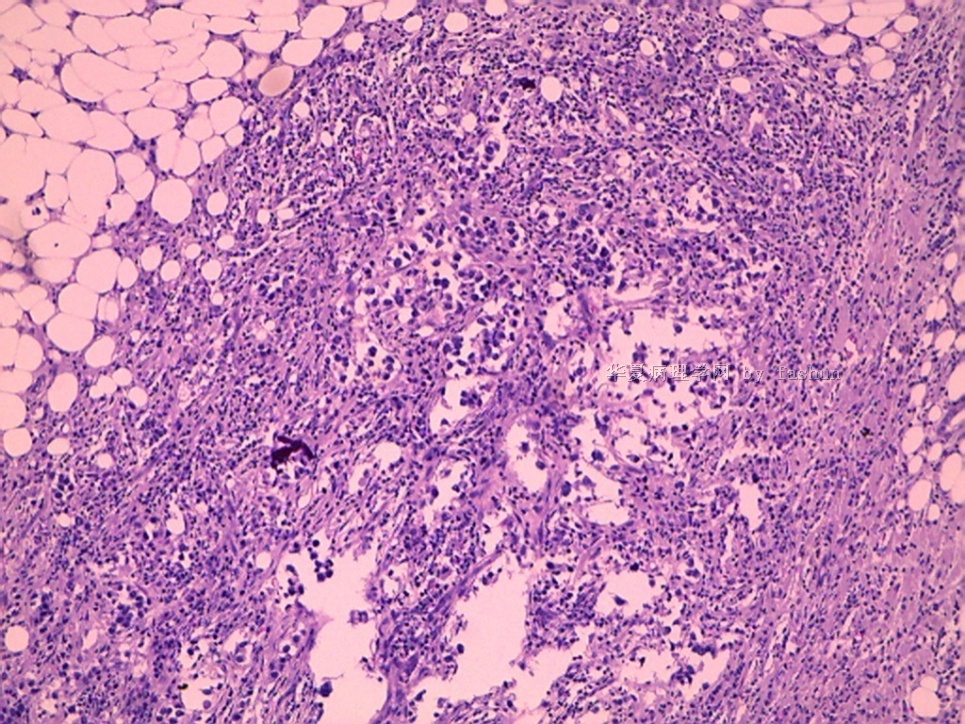
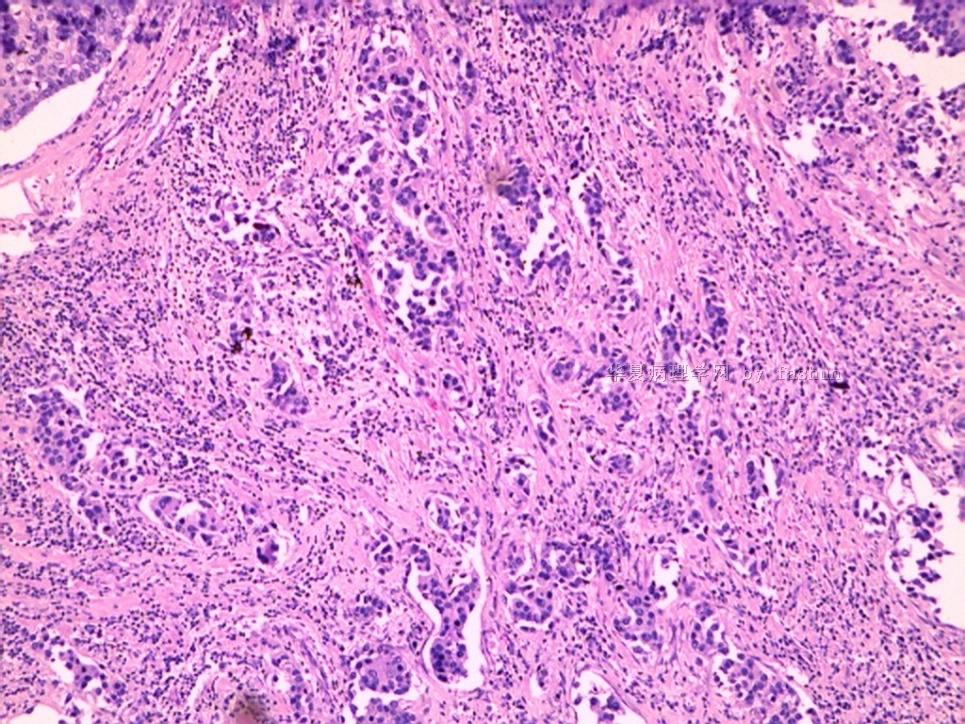
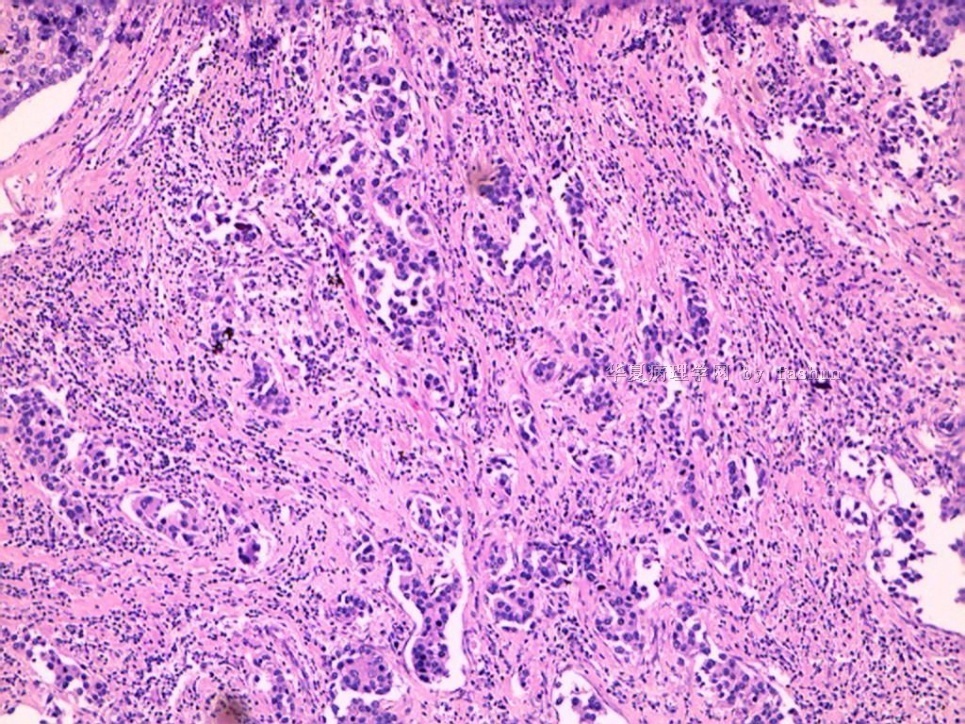
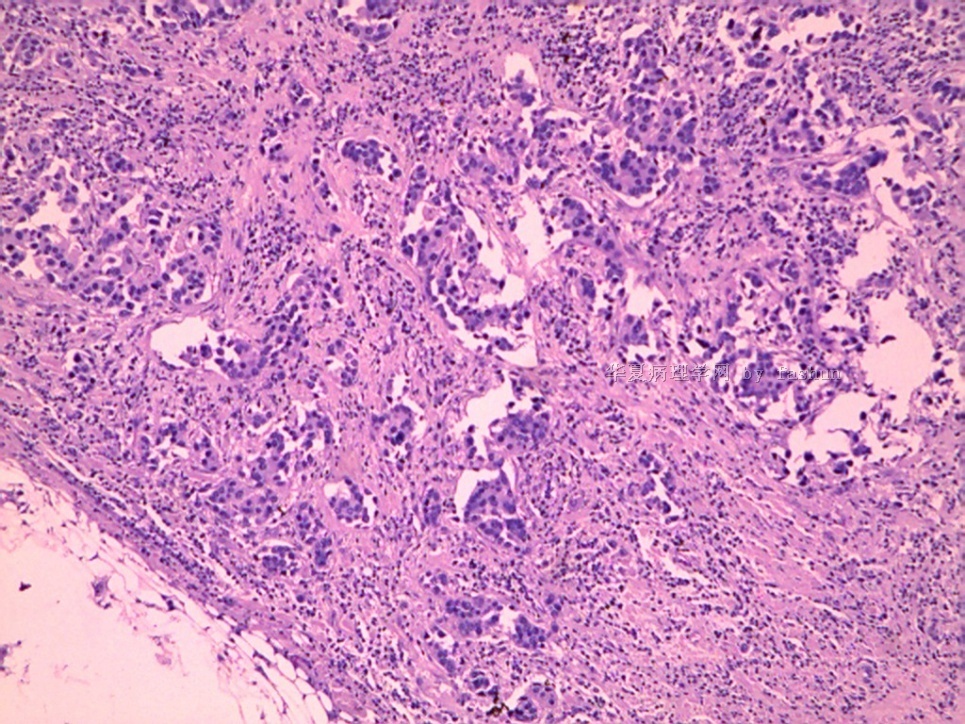
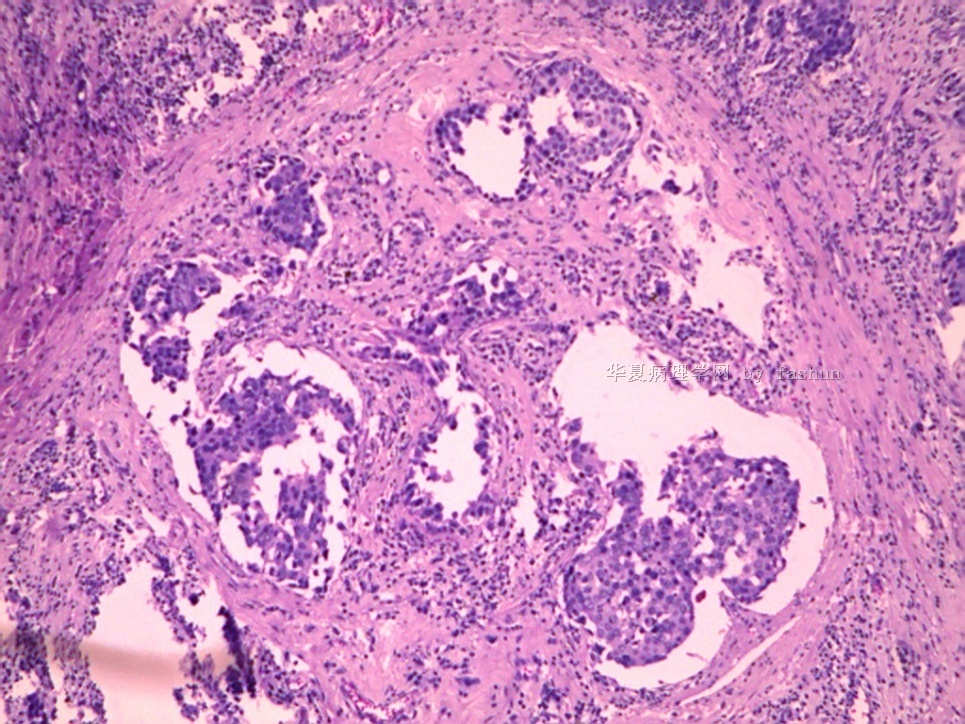
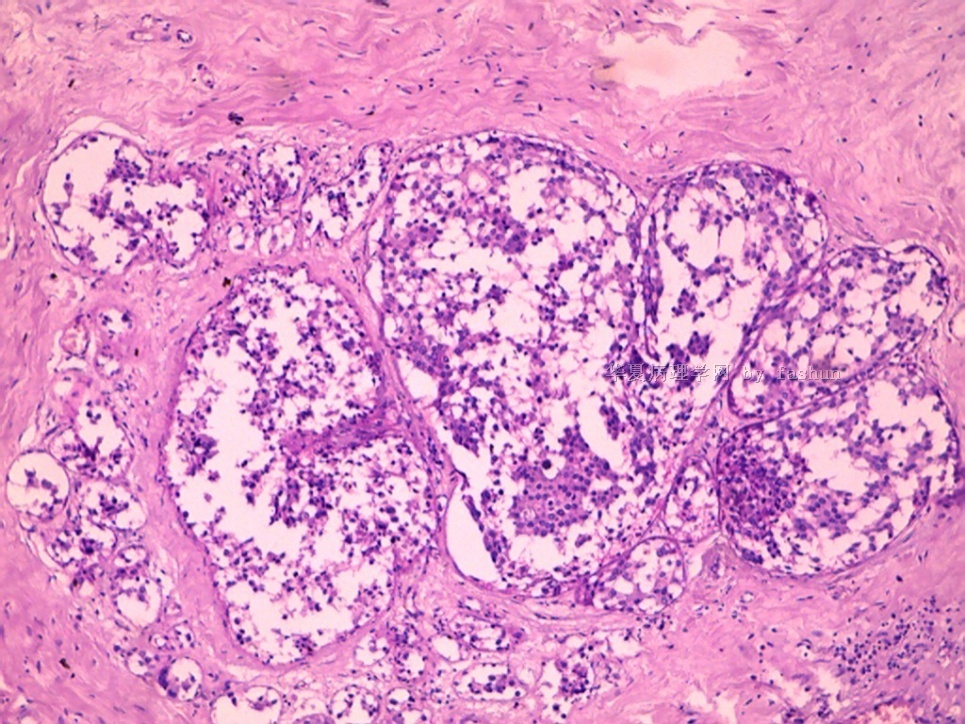
- B2890乳腺肿块
 图1
图1 图2
图2 图3
图3 图4
图4 图5
图5 图6
图6 图7
图7 图8
图8 图9
图9 图10
图10 图11
图11
| 姓 名: | ××× | 性别: | 年龄: | 40 | |
| 标本名称: | |||||
| 简要病史: | |||||
| 肉眼检查: | 左乳肿块 | ||||
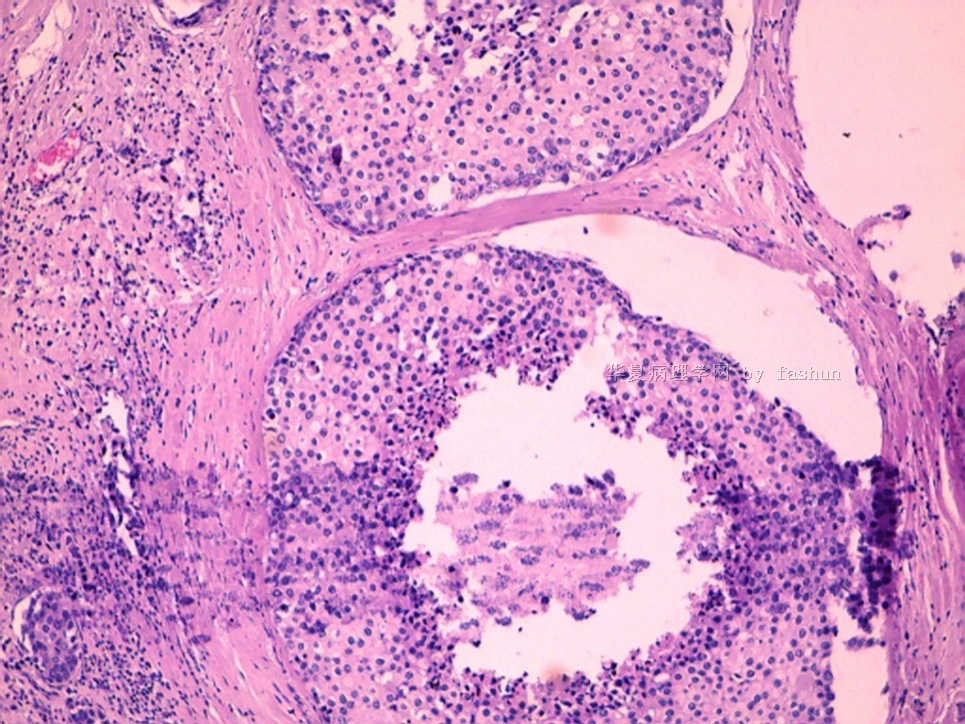
标签:冰冻 DCIS
相关帖子
- • 左乳腺肿物
- • 乳腺癌?
- • 乳腺肿物
- • 乳腺肿物
- • 左乳癌标本乳头一个导管内的病变
- • 乳腺两个相邻导管内的病变
- • 乳腺肿物,请各位老师帮忙会诊
- • 女 46岁发现左乳腺肿块一月余
- • 乳腺肿物
- • 乳腺肿物
×参考诊断
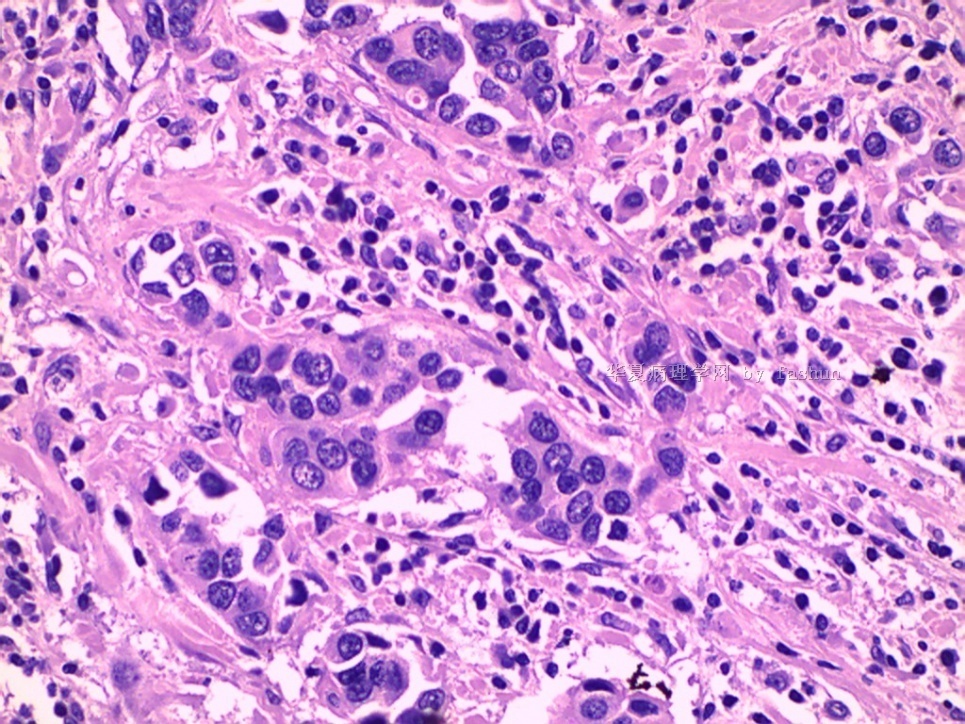
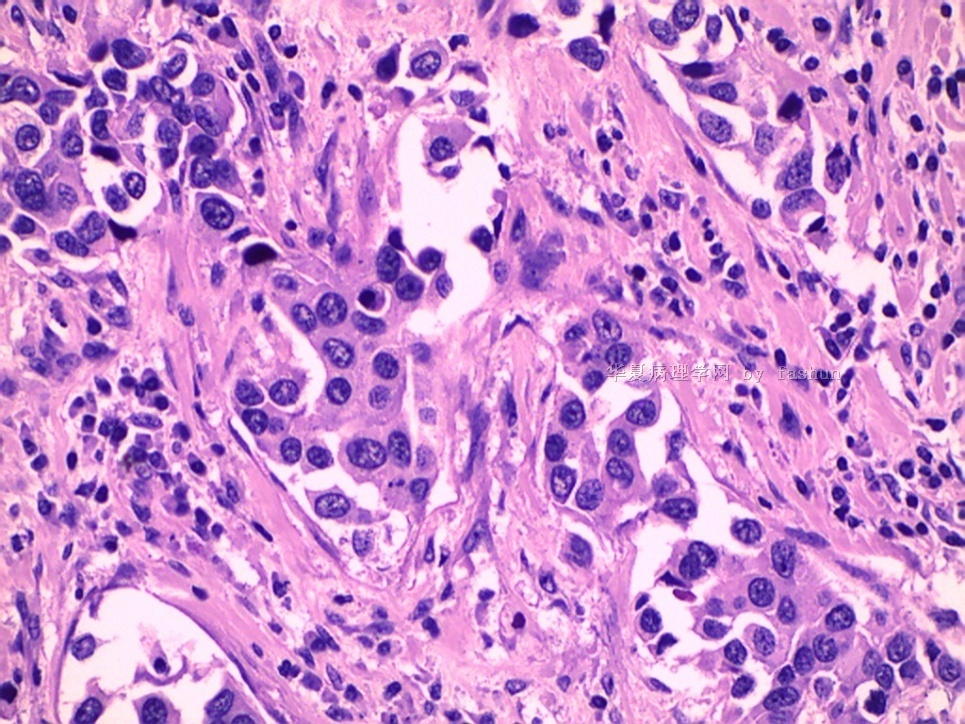
冰冻:导管原位癌
常规取材发现浸润
| 以下是引用cqzhao在2010-10-26 19:41:00的发言:
Interesting. I did not remember that I did any breast frozen for diagnosis.
|
i agree with you.
the following passage is cited from sternberg's diagnostic surgical patholgy
In recent years, owing to changes in clinical practice, the use of the frozen section to diagnose mammary carcinoma has declined. Malignancy is usually diagnosed by either core needle biopsy or open excisional biopsy of ambulatory patients. The need to consider treatment alternatives precludes the use of frozen section diagnosis immediately before definitive treatment (2). Frozen sections may be appropriate for the confirmation of a cytologic diagnosis of carcinoma or the evaluation of surgical margins. If frozen section is undertaken and any doubt arises about the diagnosis, a final decision should be deferred until processed tissue is available. Difficulties are usually attributable to sampling errors, technical problems, or occasionally true histologic misinterpretation. Errors in interpretation arise particularly with sclerosing lesions (sclerosing adenosis, radial scar, ductal adenoma), epithelial hyperplasia, papillary lesions, and fat necrosis. The diagnosis of in situ carcinoma can also cause problems, not only because it may be difficult to distinguish from benign epithelial hyperplasia but also because stromal invasion cannot always be excluded in the small sample usually examined.
| 以下是引用笃行者在2010-10-20 20:36:00的发言:
我们医院乳腺病例几乎都做术中冰冻,无论良恶性。 临床医生的目的一方面是为了决定手术范围(对于术前考虑恶性的),另一方面也是为了早知道结果(对于术前考虑良性的病人)。我们多次提出反对但无济于事。 好在我们的临床医生大部分都有丰富的经验,并且术前病人几乎都会做钼靶照相和B超检查,良恶性术前都判断个八九不离十,一旦病理诊断和他们的预料有出入他们会打电话问的,遇到这种情况我们也会主动和手术台联系的。好在是我院大部分乳腺癌病人都做保乳术,所以也给我们减轻了一部分压力。 即使这样,除非病变十分典型,且病理诊断与术前的临床诊断不矛盾,才直接写出诊断。否则我们常常在提出倾向性意见后,再加上“最后诊断请待常规病理”或“待常规病理进一步确诊”等字样,来保护自己。 |
Interesting. I did not remember that I did any breast frozen for diagnosis.
我们医院乳腺病例几乎都做术中冰冻,无论良恶性。
临床医生的目的一方面是为了决定手术范围(对于术前考虑恶性的),另一方面也是为了早知道结果(对于术前考虑良性的病人)。我们多次提出反对但无济于事。
好在我们的临床医生大部分都有丰富的经验,并且术前病人几乎都会做钼靶照相和B超检查,良恶性术前都判断个八九不离十,一旦病理诊断和他们的预料有出入他们会打电话问的,遇到这种情况我们也会主动和手术台联系的。好在是我院大部分乳腺癌病人都做保乳术,所以也给我们减轻了一部分压力。
即使这样,除非病变十分典型,且病理诊断与术前的临床诊断不矛盾,才直接写出诊断。否则我们常常在提出倾向性意见后,再加上“最后诊断请待常规病理”或“待常规病理进一步确诊”等字样,来保护自己。

- 博学之,审问之,慎思之,明辨之,笃行之。
-
Thank you for sharing above photos. Clearly it is IDC and DCIS now. The surgeon did not give you the invasive area for frozen. It is good evidence that open surgery with frozen is not a good method for breast lesions. This method has not been used for about 30 year in the usa. Do not understand our surgeons still love this method in China











