
























| 图片: | |
|---|---|
| 名称: | |
| 描述: | |
- 右腋中线结节,左侧会阴结节
-
本帖最后由 于 2010-08-09 08:29:00 编辑
临床病理特点:
1)男性病人,50岁。
2)全身皮下多发性病灶、脑“囊肿”
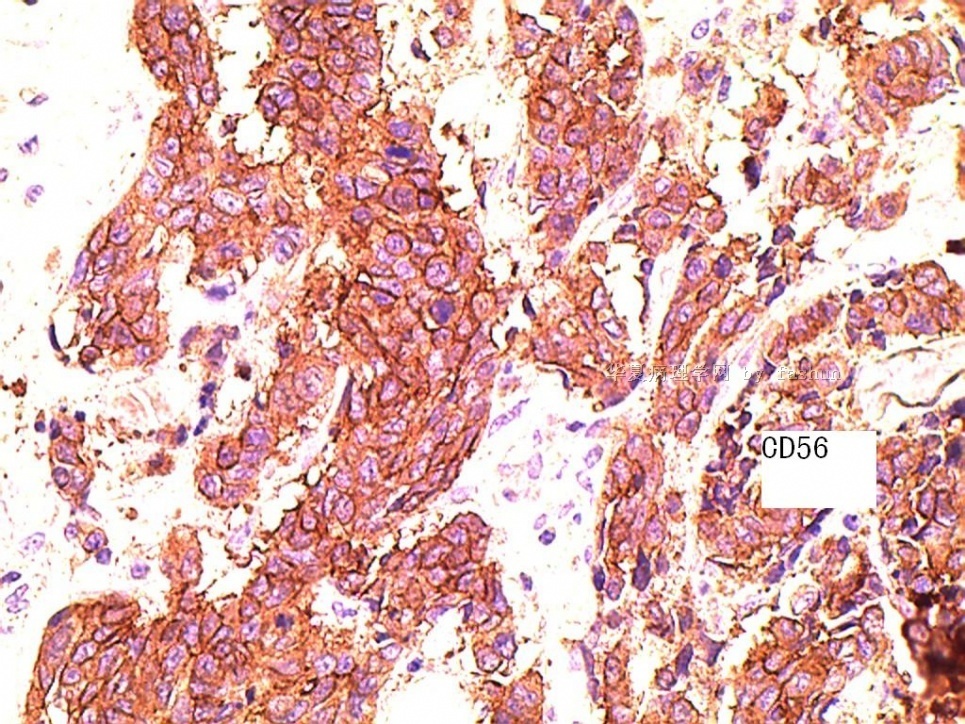
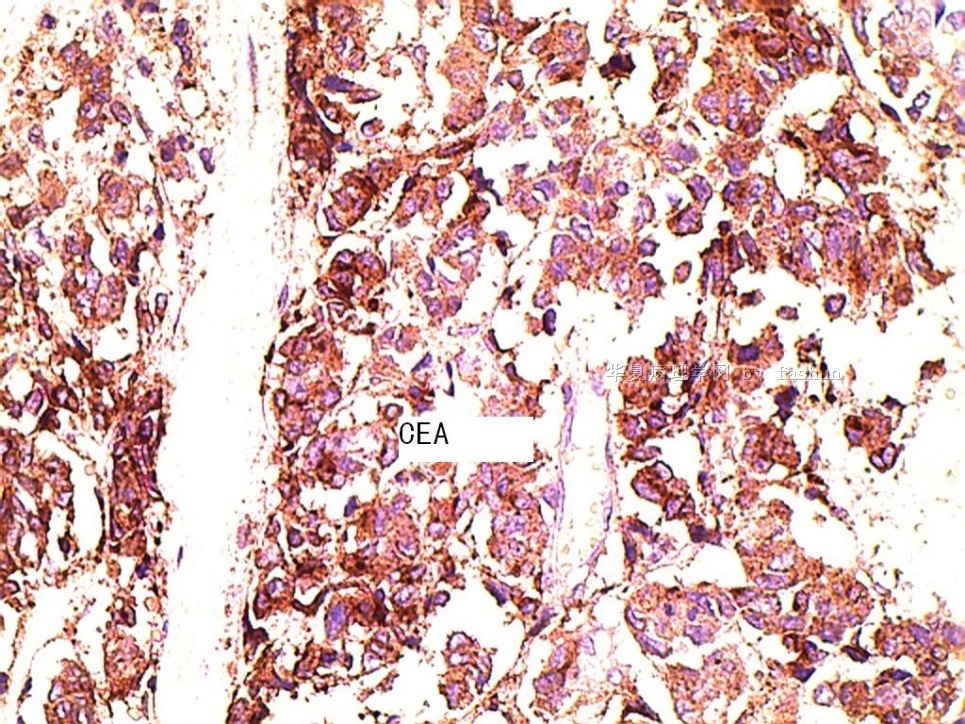
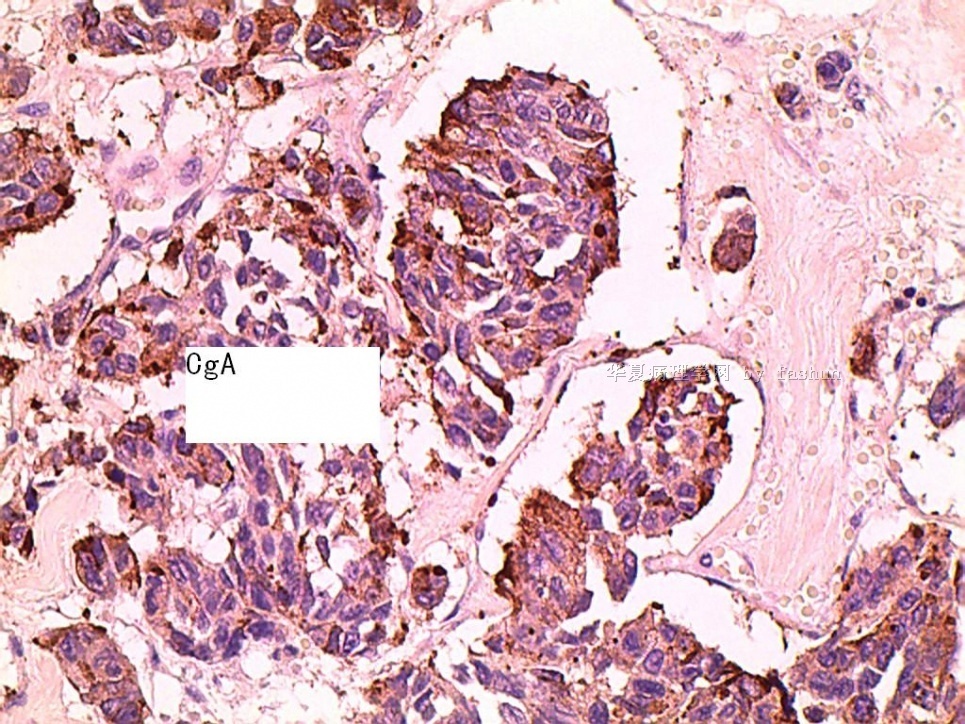
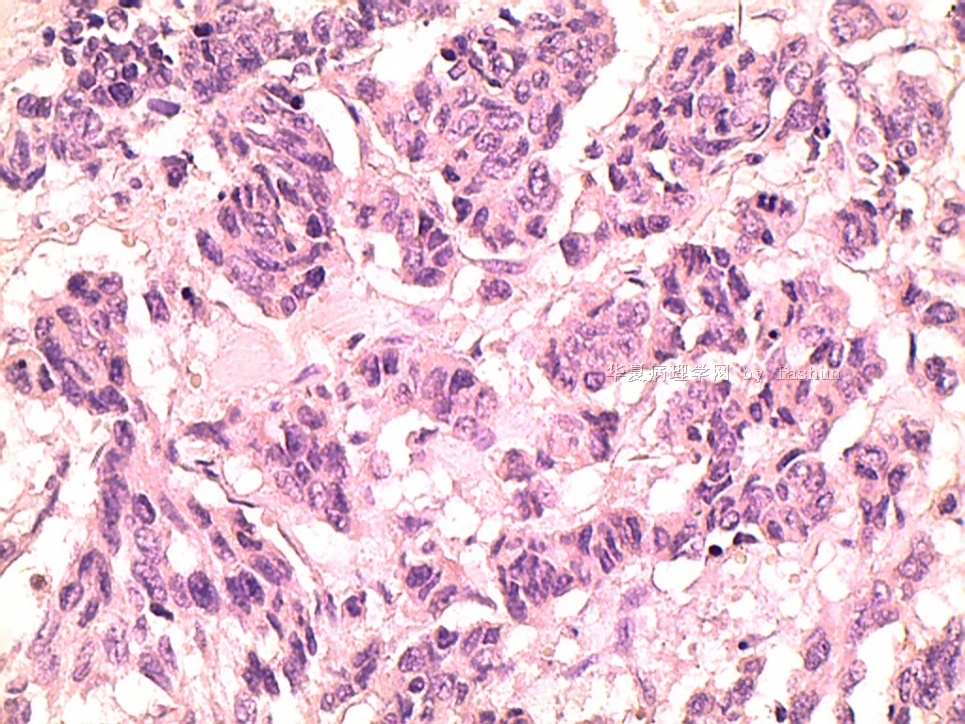
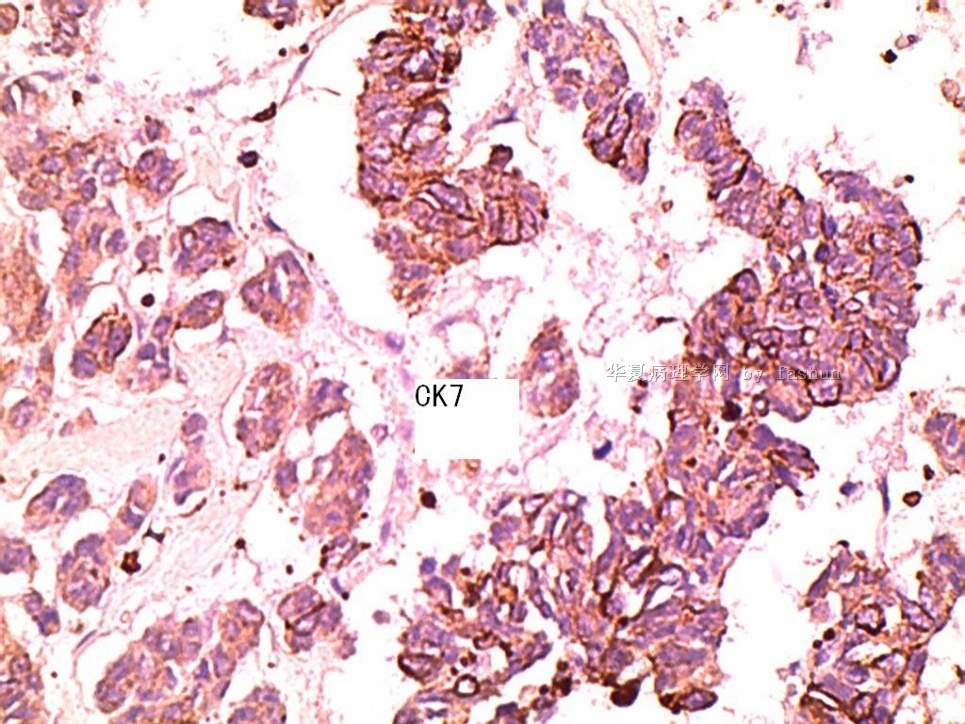
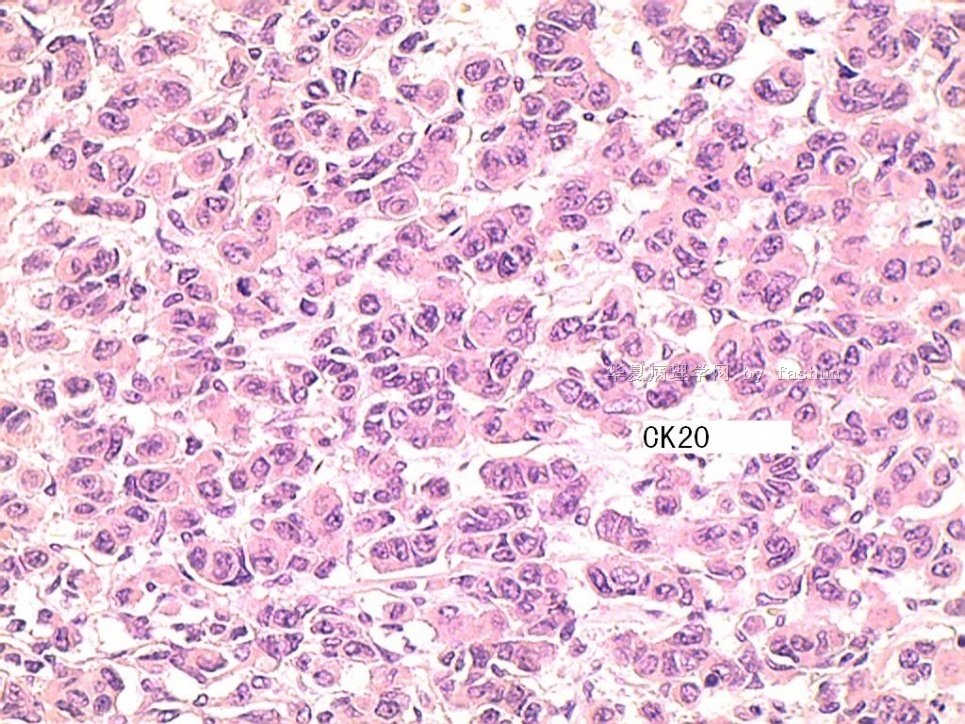
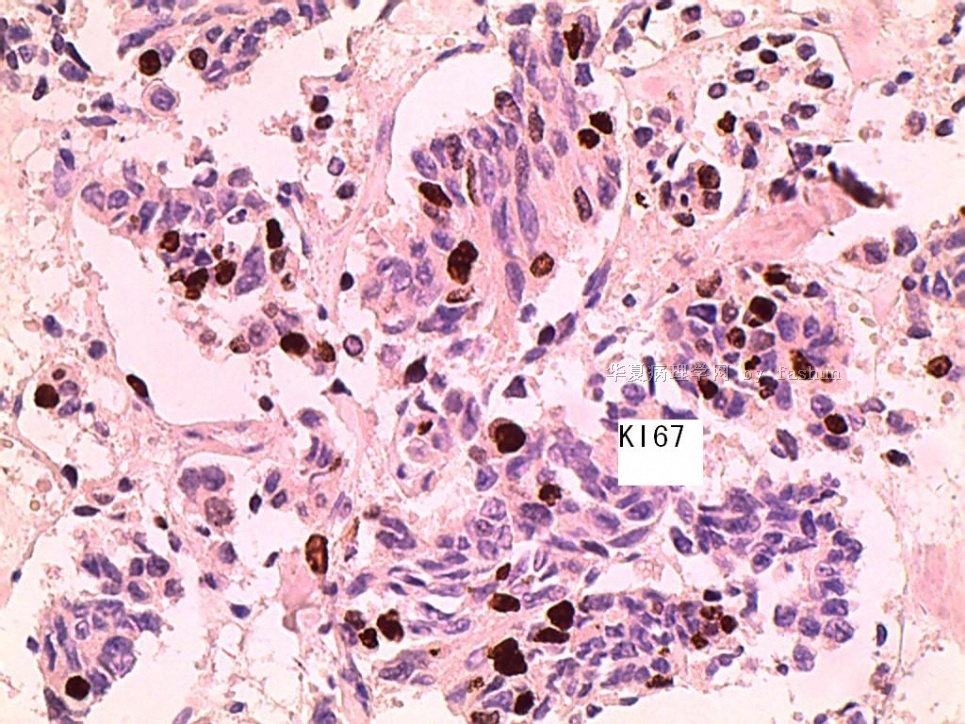
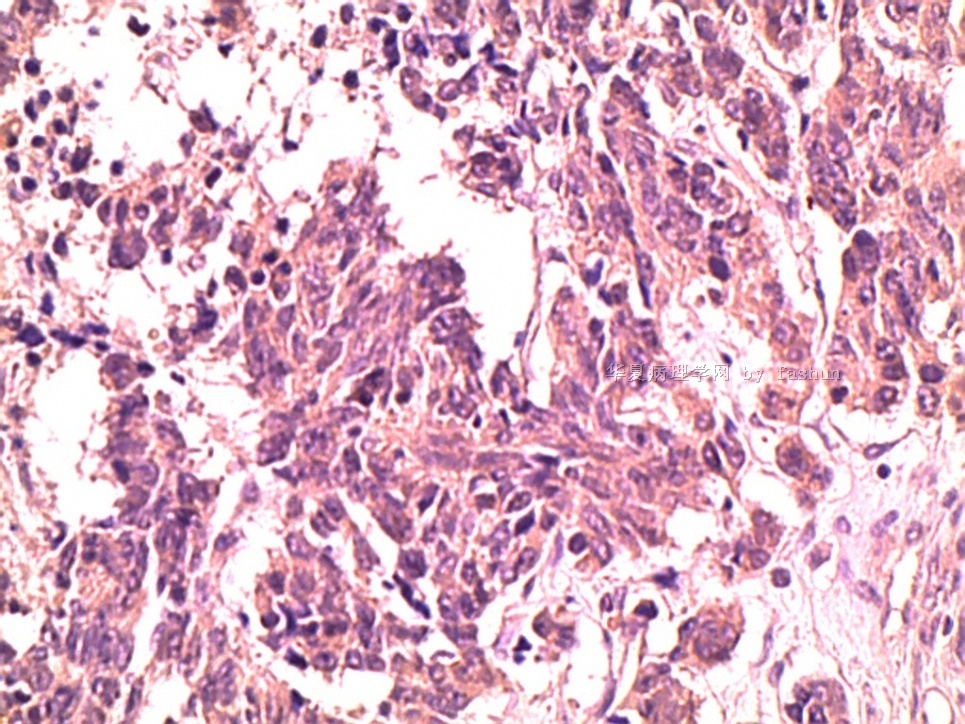
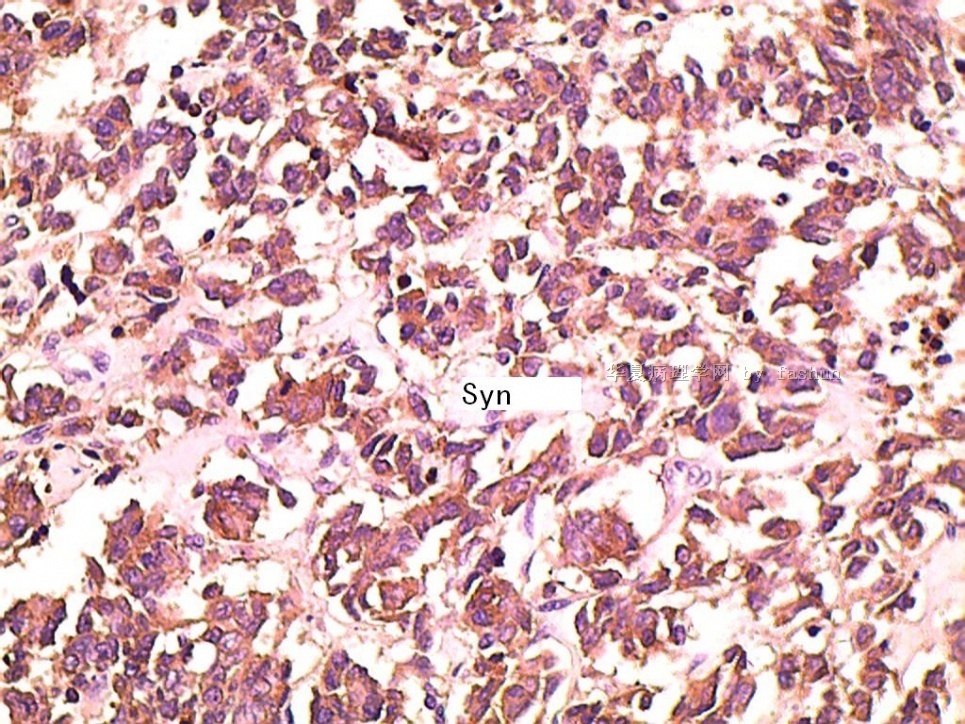
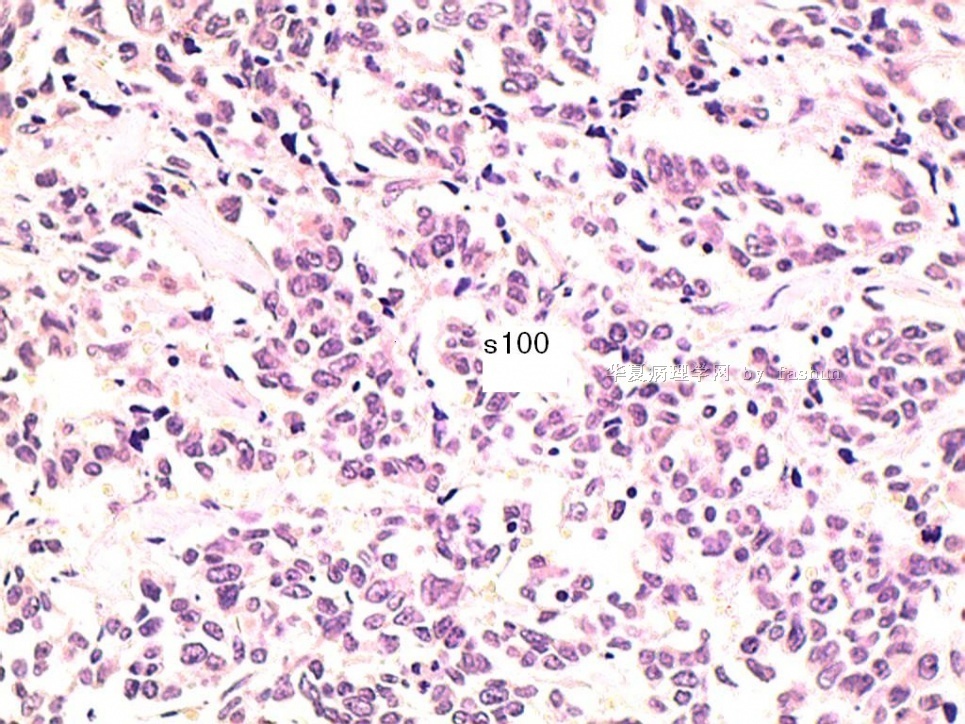
3)镜下低分化恶性肿瘤、肿瘤性坏死明显。
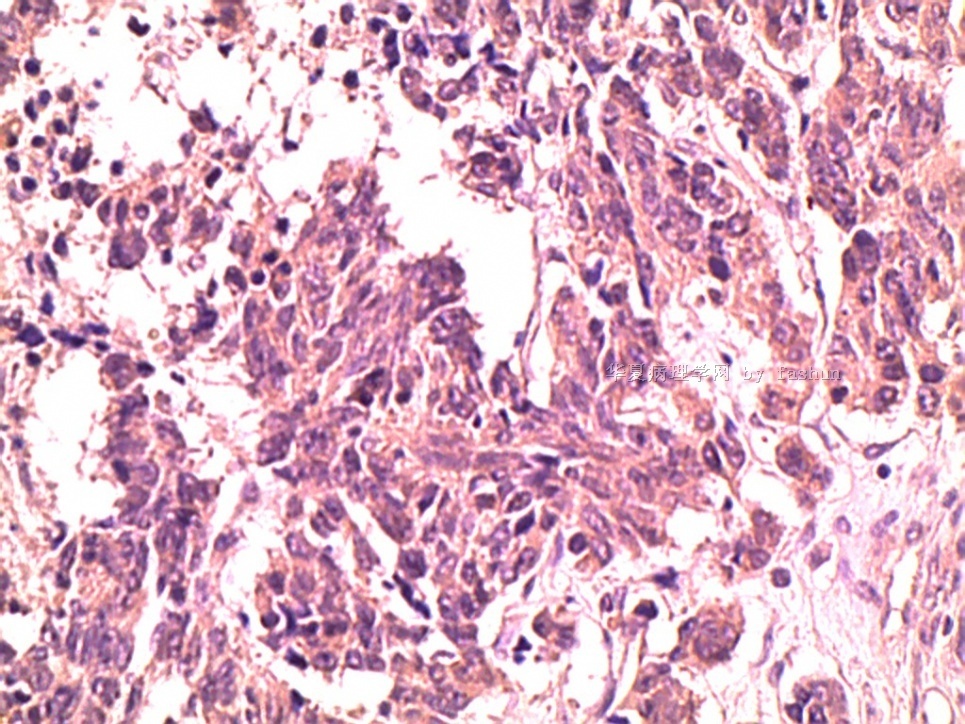
4)肿瘤主要为实体巢、梁、条索;间质血管丰富,
5)细胞多形性,梭形、圆形、不规则形,细胞质比较丰富、嗜酸性颗粒状;
6)少数细胞条束内似有鳞状分化,
7)无腺样结构、无黏液及特殊结构;
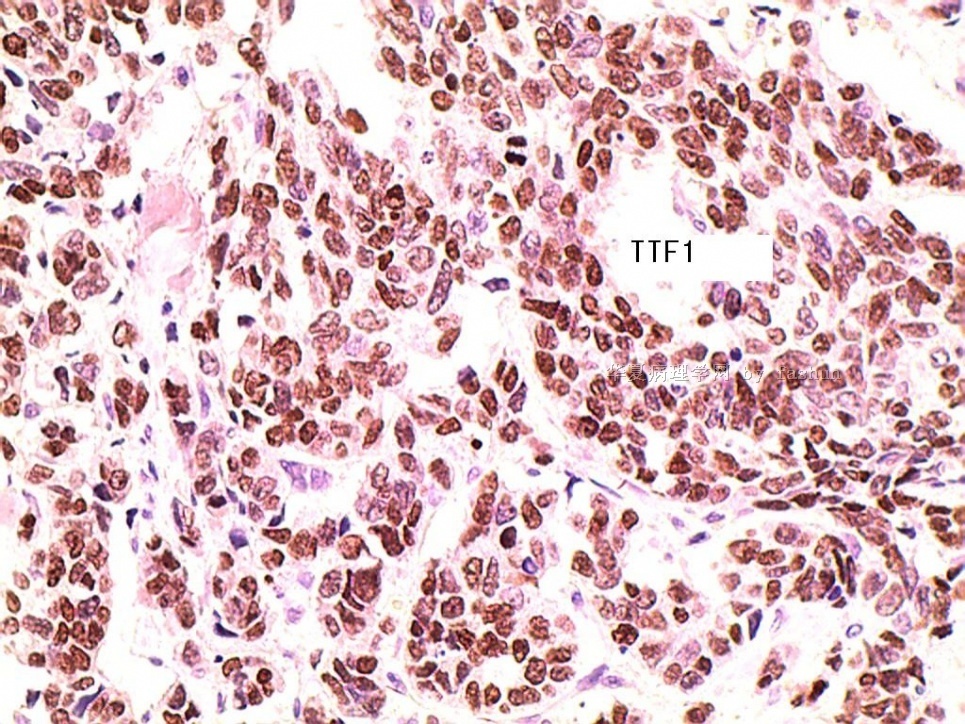
诊断首先考虑:低分化神经内分泌癌(大细胞性或混合性)
其来源:最可能来自肺。
明确要靠影像学检查。
如除外转移性,要考虑皮肤附近来源。但不是“Merkel 细胞癌”。

- xljin8
-
xfyz690524 离线

- 帖子:27
- 粉蓝豆:2016
- 经验:31
- 注册时间:2007-10-30
- 加关注 | 发消息
-
本帖最后由 于 2010-08-12 23:51:00 编辑
- Çağatay Erşahin, MD, PhD
- Department of Pathology, Loyola University Medical Center, Maywood, Illinois, cersahin@lumc.edu, Department of Pathology, Magee-Women\s Hospital of University of Pittsburgh Medical Center, Pittsburgh, Pennsylvania
- Rohit Bhargava, MD
查到文献如下,分享参考。
Napsin A and thyroid transcription factor-1 expression in carcinomas of the lung, breast, pancreas, colon, kidney, thyroid, and malignant mesothelioma
Auteur(s) / Author(s)
BISHOP Justin A. (1) ; SHARMA Rajni (1) ; ILLEI Peter B. (1) ;
Affiliation(s) du ou des auteurs / Author(s) Affiliation(s)
(1) Department of Pathology, The Johns Hopkins Medical Institutions, Baltimore, MD 21231, ETATS-UNIS
Résumé / Abstract
Recent advances in the treatment of pulmonary adenocarcinoma have increased the need for accurate typing of non-small cell carcinomas. Immunohistochemistry for thyroid transcription factor-1 is widely used in the diagnosis of pulmonary adenocarcinomas because it marks approximately 75% of lung adenocarcinomas and is negative in most squamous cell carcinomas and adenocarcinomas of other organs. Napsin A is an aspartic proteinase involved in the maturation of surfactant protein B. It is detected in the cytoplasm of type 2 pneumocytes and alveolar macrophages and is a putative marker for pulmonary adenocarcinomas. We performed immunohistochemistry for napsin A and thyroid transcription factor-1 using tissue microarrays of 95 adenocarcinomas, 48 squamous cell carcinomas, 6 neuroendocrine tumors of the lung, as well as 5 colonic, 31 pancreatic, and 17 breast adenocarcinomas, 38 malignant mesotheliomas; 118 renal cell carcinomas, and 81 thyroid tumors. The tissue microarrays also included 15 different benign tissues. Pulmonary adenocarcinomas were napsin A positive in 79 (83%) of 95 cases compared with 69 (73%) of 95 cases that were thyroid transcription factor-1 positive. There were 13 napsin A-positive/thyroid transcription factor-1-negative and 2 thyroid transcription factor-1-positive/napsin A-negative tumors, increasing the number of cases that were positive with at least one of the markers to 81 (85%) of 95. The limited number of neuroendocrine tumors tested was napsin A negative. All squamous cell carcinomas, adenocarcinomas of the colon, pancreas and breast, and mesotheliomas were negative for both markers. Of the renal tumors, napsin A was positive in most of papillary renal cell carcinomas (79%), about one third (34%) of clear cell renal cell carcinomas, and in a single case of chromophobe renal cell carcinoma (3%). In the thyroid, only 2 cases of papillary thyroid carcinoma (5%), both with tall cell morphology, were positive for napsin A, whereas all other papillary and follicular carcinomas were negative. As expected, all renal tumors were thyroid transcription factor-1 negative, and all thyroid tumors, except for one papillary carcinoma, were thyroid transcription factor-1 positive. Napsin A is a sensitive marker for pulmonary adenocarcinoma and is also expressed in a subset of renal cell carcinomas, particularly of the papillary type, as well as in rare cases of papillary thyroid carcinomas. The combined use of napsin A and thyroid transcription factor-I results in improved sensitivity and specificity for identifying pulmonary adenocarcinoma in primary lung tumors and in a metastatic setting.
Revue / Journal Title
Human pathology ISSN 0046-8177 CODEN HPCQA4
Expression of Thyroid Transcription Factor-1 in Colorectal Carcinoma
Xu, Bo MD, PhD; Thong, Nguyen MD; Tan, Dongfeng MD; Khoury, Thaer MD
Thyroid transcription factor 1 expression in ovarian carcinomas is an independent prognostic factor☆
Received 27 April 2009; received in revised form 9 September 2009; accepted 24 September 2009. published online 11 December 2009.
Summary
Tthyroid transcription factor 1 is a marker of lung and thyroid carcinomas, but thyroid transcription factor 1 immunoreactivity is seen in other malignancies. We examined the incidence of thyroid transcription factor 1 expression in gynecologic tumors in Japanese patients, and we further evaluated the presence of epidermal growth factor receptor mutations in thyroid transcription factor 1–positive gynecologic malignancies. A total of 186 patient samples collected at our hospitals between 1991 and 2006 were analyzed, and these specimens consisted of 83 ovarian carcinomas, 55 endometrioid endometrial adenocarcinomas of the uterus, 28 cervical adenocarcinomas of the uterus, and 20 leiomyosarcomas of the uterus. Thyroid transcription factor 1 expression was assessed by immunohistochemistry. The presence of epidermal growth factor receptor mutations was investigated by polymerase chain reaction analyses. Thyroid transcription factor 1 was detected in the nuclei of 11 ovarian carcinomas (13%) and 5 endometrioid adenocarcinomas (10%) of the uterus. In patients with ovarian carcinoma, thyroid transcription factor 1 staining was associated with significantly improved progression-free (P = .017) and overall survival (P = .017) using univariate analysis. Multivariate analysis identified thyroid transcription factor 1 expression as an independent prognostic factor for ovarian cancer (P = .0467). No epidermal growth factor receptor mutations were found in our study. Thyroid transcription factor 1 is expressed with relatively low frequencies in gynecologic malignancies, but thyroid transcription factor 1 expression confers a better prognosis in patients with ovarian cancer. No epidermal growth factor receptor mutations were found in the thyroid transcription factor 1–positive gynecologic malignancies, and we were unable to establish a relationship between epidermal growth factor receptor mutations and thyroid transcription factor 1 immunopositivity, as was previously shown for lung cancer.
Abstract
Thyroid transcription factor-1 (TTF-1) is a member of the homeodomain transcription family expressed in epithelial cells of the thyroid and lung. Although nuclear TTF-1 is generally considered a specific marker for lung and thyroid neoplasms, it has been reported to be positive in other types of tumors including colorectal carcinoma (CRC). During metastatic adenocarcinoma workup for patients who had a history of CRC, we identified 4 positive TTF-1 cases using clone 8G7G3/1. Three of the 4 corresponding primary carcinomas were also positive for TTF-1. Therefore, we sought to retrospectively investigate the expression of TTF-1 in 100 CRC cases constructed in tissue microarray blocks and whole tissue sections of the 4 primary tumors corresponding to the 4 positive metastases. In tissue microarray cases, all cases had negative nuclear staining. Our results suggest that during immunohistochemical workup for adenocarcinoma, especially when the differential diagnosis includes the lung and CRC, TTF-1 results should be interpreted with caution as a small percentage of CRC expresses this marker. Positive nuclear TTF-1 in a metastatic carcinoma does not rule out CRC primary. Clinicopathologic correlation, tumor morphology, and a panel of immunohistochemical markers are essential to render the correct diagnosis.
Thyroid Transcription Factor-1 and “Basal Marker”—Expressing Small Cell Carcinoma of the Breast
Abstract
Small cell carcinoma of the breast is a very rare entity that is histologically indistinguishable from small cell carcinomas of other organs. The presence of an in situ component is the most important feature that indicates the primary nature of the breast tumor. Thyroid transcription factor-1 (TTF-1) is a marker specific to lung and thyroid but is also expressed in small cell carcinoma of pulmonary and extrapulmonary origin. TTF-1 expression in breast small cell carcinoma has been reported only rarely. This reported case is unique because of the characteristic morphological features and immunohistochemical profile. The invasive tumor demonstrated neuroendocrine differentiation morphologically and immunohistochemically, expressed by TTF-1, EGFR, and basal-type cytokeratins. An unequivocal in situ component was identified intimately admixed with the invasive carcinoma. To the authors’ knowledge, this is the first report of breast small cell carcinoma showing the expression of “basal markers.”
Mod Pathol. 2000 Mar;13(3):238-42.
Thyroid transcription factor-1 is expressed in extrapulmonary small cell carcinomas but not in other extrapulmonary neuroendocrine tumors.
Agoff SN, Lamps LW, Philip AT, Amin MB, Schmidt RA, True LD, Folpe AL.
Department of Pathology, University of Washington, Seattle, USA.
Abstract
Thyroid transcription factor-1 (TTF-1) is a nuclear homeodomain transcription factor that is expressed in the developing thyroid, respiratory epithelium, and diencephalon. TTF-1 is thought to be expressed specifically in pulmonary or thyroid neoplasms, and it is expressed in a significant subset of pulmonary non-small cell carcinomas, small cell carcinomas, and carcinoids but not in nonpulmonary, non-small cell carcinomas. Neuroendocrine tumors from sites other than the lung have not been evaluated for TFF-1 expression. We examined TFF-1 expression using immunohistochemistry on formalin-fixed, paraffin-embedded sections of 49 gastrointestinal carcinoids; 15 pancreatic islet cell tumors; 21 paragangliomas; 8 medullary thyroid carcinomas; 7 small cell carcinomas of the uterine cervix; 4 prostate, 4 bladder, and 6 Merkel cell (primary cutaneous neuroendocrine) carcinomas; and 1 renal carcinoma No gastrointestinal carcinoid tumor, pancreatic islet cell tumor, paraganglioma, or Merkel cell carcinoma expressed TFF-1. All of the medullary thyroid carcinomas strongly expressed TTF-1. However, 44% of nonpulmonary small cell carcinomas were also TTF-1 positive, including four of four prostate, two of four bladder, and one of seven cervical small cell carcinomas. We conclude that TTF-1 expression is not specific for small cell carcinomas of pulmonary origin and should not be used to distinguish primary from metastatic small cell carcinomas in extrapulmonary sites. However, TTF-1 expression may be useful in distinguishing Merkel cell carcinomas and cutaneous metastasis of small cell carcinomas. Among well-differentiated neuroendocrine tumors, TTF-1 expression seems to be present only in carcinoid tumors of the lung and medullary carcinomas of the thyroid and may be of differential diagnostic value when dealing with a metastatic well-differentiated neuroendocrine tumor.











