









| 图片: | |
|---|---|
| 名称: | |
| 描述: | |
- B2757201006761乳腺快速.急!谢谢!
| 姓 名: | ××× | 性别: | female | 年龄: | 78 |
| 标本名称: | |||||
| 简要病史: | |||||
| 肉眼检查: | |||||
发现左乳包块一年余.带乳头的淡黄色组织一块最大径8CM,剖开见最大径5CM大小的灰黄色肿块部分呈囊状

名称:图1
描述:图1

名称:图2
描述:图2

名称:图3
描述:图3

名称:图4
描述:图4

名称:图5
描述:图5

名称:图6
描述:图6

名称:图7
描述:图7

名称:图8
描述:图8
标签:囊内乳头状癌

朱正龙
相关帖子
- • 乳腺肿瘤?
- • 右乳包块(镜下富于粘液)
- • 左乳肿块
- • 边界清楚的乳腺包块
- • 乳腺肿块,请会诊
- • 乳腺癌?
- • 左乳腺肿块,新加免疫组化
- • 左乳肿块,新加免疫组化
- • 乳腺包块-请会诊
- • 左乳肿块
×参考诊断
| 以下是引用cqzhao在2010-7-2 23:31:00的发言:
Dr. wy1992 alway uses the term "急!". why 急. Often I did not see your follow up result. Suggest that you please put your stains and final dx in your cases. Thanks, cz |
赵老师的建议:
wy1992医生总是说“急!”。为啥用急这个字眼呢。
可总没见后续结果呀。
所以建议,请将其IHC标记和最终诊断纳入病例讨论中。谢谢!
cz
- 王军臣
| 以下是引用cqzhao在2010-7-2 23:31:00的发言:
Dr. wy1992 alway uses the term "急!". why 急. Often I did not see your follow up result. Suggest that you please put your stains and final dx in your cases. Thanks, cz |
朱正龙
Dear Dr. wy1992 , Thank you very much for your follow up result.
Based on the morphology, your IHC, lymph node metastasis, most likely it is a encapsulated papillary ca with stromal invasion.
We will appreciate it if you can paste your stains and positive lymph node photo here.
-
本帖最后由 于 2010-07-13 09:46:00 编辑
| 以下是引用cqzhao在2010-7-11 1:26:00的发言:
Dear Dr. wy1992 , Thank you very much for your follow up result. Based on the morphology, your IHC, lymph node metastasis, most likely it is a encapsulated papillary ca with stromal invasion. We will appreciate it if you can paste your stains and positive lymph node photo here. |
名称:图1
描述:图1
名称:图2
描述:图2
名称:图3
描述:图3
名称:图4
描述:图4

名称:图5
描述:图5
名称:图6
描述:图6
名称:图7
描述:图7
名称:图8
描述:图8
朱正龙
-
本帖最后由 于 2010-07-13 21:37:00 编辑
学习:
谢谢楼主和老师们的评议。
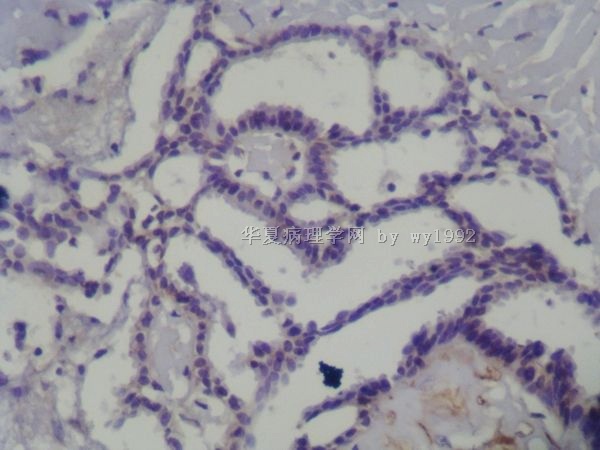
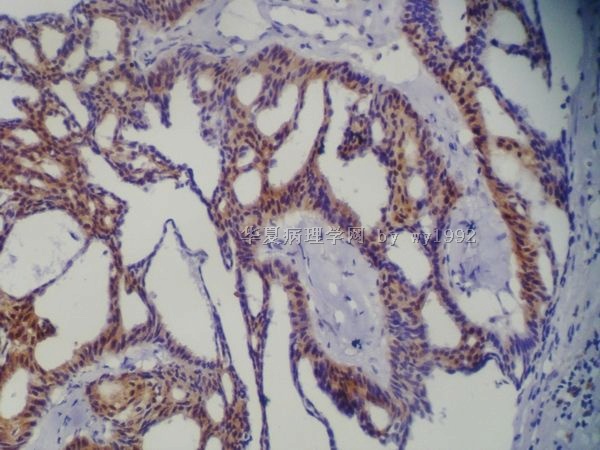
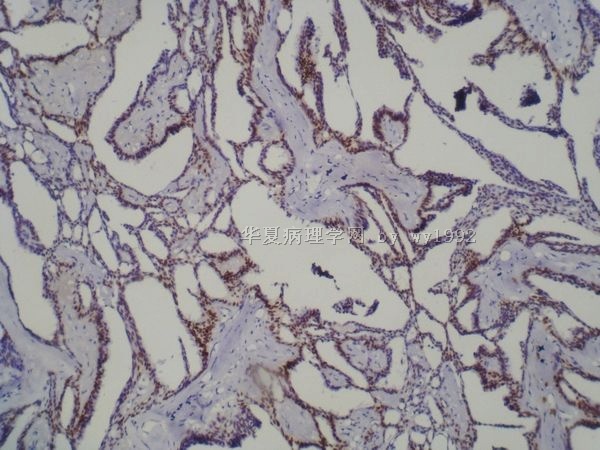
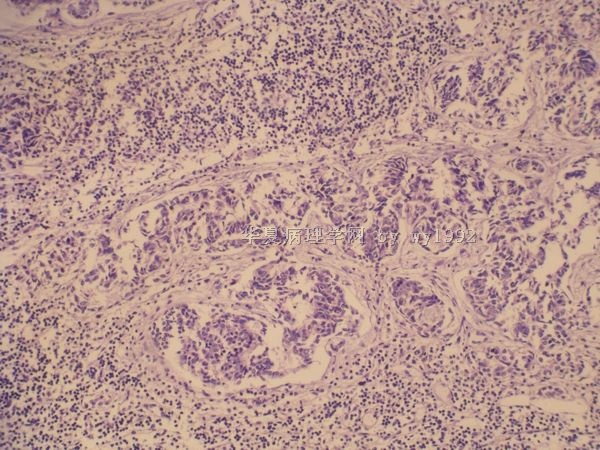
本例首页提供的常规染色图片,多为囊内部分肿瘤组织,也可见少量交界区图像。如果整个取材标本的均为如上组织像,可能的鉴别诊断有伴有非典型增生的导管内乳头状瘤、乳头状导管内原位癌、Encapsulated Papillary Carcinomas(有无伴有浸润性癌成分现在还不能下结论)等。
本例出现淋巴结转移,文献报道囊内乳头状癌也可伴有淋巴结转移,学习后感到该种肿瘤的命名来源于形态学特点但是不能完全反映肿瘤的生物学行为,可能全面的取材和描述对于诊断很重要。
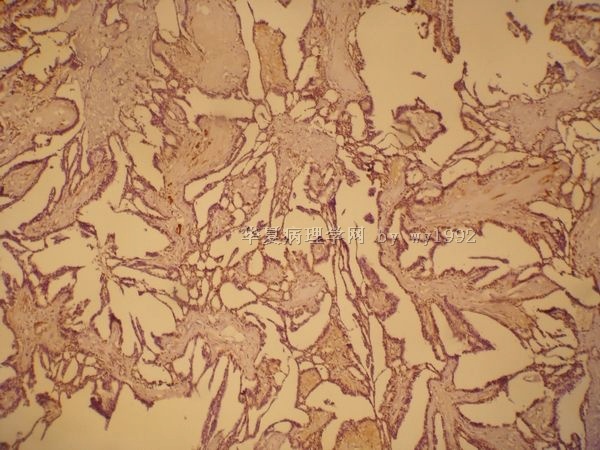
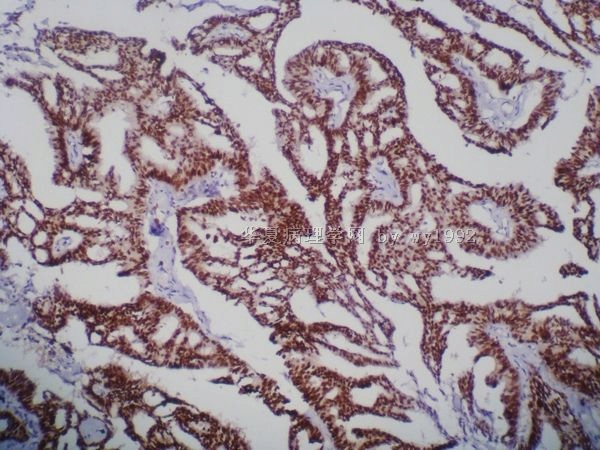
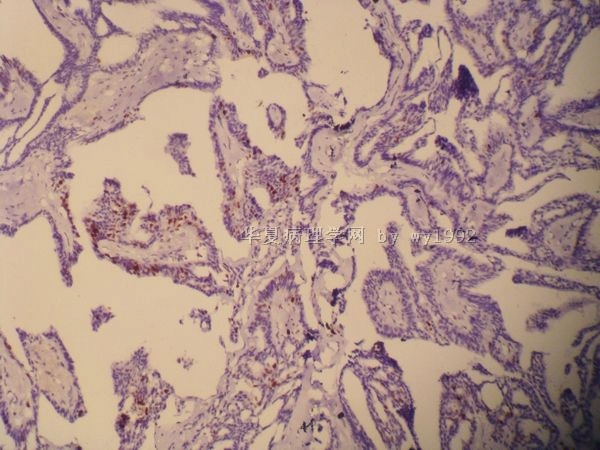
本例免疫组化结果:ER(+),PR(+),CALPONIN-/+?,P63不规则核浆型(+),Ki-67灶性乳头上皮(+)。
P63的特殊胞浆型表达在能够排除非特性染色的情况下,可参考以下病例中的文献,很有趣。
http://www.ipathology.cn/forum/forum_display.asp?classcode=176&keyno=259020&pageno=3
问题:请教如何评判本例的P63结果,K—67的较低阳性阳性率可以提示什么?
Are Encapsulated Papillary Carcinomas of the Breast In Situ or Invasive?
A Basement Membrane Study of 27 Cases
1. Nicole Nicosia Esposito, MD,
2. David J. Dabbs, MD and
3. Rohit Bhargava, MD
+ Author Affiliations
1. From the Department of Pathology, Magee-Womens Hospital of the University of Pittsburgh, Pittsburgh, PA
Abstract
Encapsulated papillary carcinoma (EPC) of the breast is traditionally considered a variant of ductal carcinoma in situ (DCIS). However, recent studies show EPCs lack myoepithelial cells at their periphery, leading some to conclude that EPCs are invasive. We used a robust collagen type IV immunohistochemical procedure to assess invasion in 21 cases of pure EPC and 6 EPCs with adjacent invasive ductal carcinoma (IDC) and compared these results with those for papilloma, DCIS, and IDC. Moderate to intense collagen type IV expression was seen in all EPCs and was absent or decreased in all IDCs. All patients with pure EPC had negative axillary nodes with the exception of 1 who had a micrometastasis, and all were alive with no evidence of disease at follow-up (mean, 40.4 months). EPCs are in situ carcinomas with an excellent prognosis and can be managed with local therapy with or without sentinel lymph node biopsy.
Key Words:
Encapsulated papillary carcinoma (EPC) of the breast, synonymous with intracystic or encysted papillary carcinoma, is traditionally considered a variant of ductal carcinoma in situ (DCIS).1 It represents approximately 0.5% to 2% of all breast cancers and typically occurs in postmenopausal women.2,3 EPC is characterized by papillary carcinoma within a well-circumscribed cystic or distended duct with cytologic features akin to papillary DCIS. Unlike papillary DCIS, however, it has recently been demonstrated that these lesions lack myoepithelial cells at their periphery, leading some authors to conclude that EPCs are, in fact, invasive carcinomas with an expansile growth pattern.4,5 In support of this conclusion, 1 study reported lung metastases developing in a patient after a diagnosis of EPC,2 and another reported 2 cases with axillary lymph node micrometastases.6
Immunohistochemical detection of myoepithelial cells at the periphery of lesional epithelium has long been used for determination of invasion in breast pathology.7 An alternative approach for assessment of invasion is immunohistochemical detection of the basement membrane. The most extensively studied proteins that constitute the basal lamina component of the basement membrane are type IV collagen and laminin.8 Immunohistochemical studies targeting these proteins have generally demonstrated linear and continuous basement membranes in benign and in situ lesions and discontinuous or absent expression in invasive carcinomas.9–11
Given the current debate regarding the invasive status of EPCs and the lack of published reports on basement membrane expression in these lesions, the aims of the present study were to determine whether encapsulated papillary carcinomas are invasive on the basis of immunohistochemical detection of basement membrane proteins and to compare these results with lymph node status and patient outcome.
Materials and Methods
Case Selection and Review
A retrospective search of the pathology database was performed for this institutional review board–approved study. Cases diagnosed as “encapsulated papillary carcinoma,” “intracystic papillary carcinoma,” or “encysted papillary carcinoma” were retrieved. This resulted in 21 cases of pure EPC (without “frank” invasion) and 6 cases of EPC with an associated invasive carcinoma. In addition, 18 benign and atypical papillomas, 7 solid papillary carcinomas (SPCs), 34 cases of DCIS, and 10 invasive ductal carcinomas (IDCs), including 6 associated with an EPC and 1 associated with an SPC, were included for comparison analysis.
All H&E-stained slides and corresponding pathology reports from each case were reviewed by 2 pathologists (N.N.E. and R.B.). All cases were classified using recently described criteria.1 Histopathologic features, including size, nuclear grade, and mitotic rate, were noted. The mitotic index was calculating by counting 10 high-power fields (HPF) on a Leica DMLS light microscope (Leica Microsystems, Wetzlar, Germany) with a 40× objective and field diameter of 0.50 mm.
To assess for the possibility of an occult microinvasive carcinoma that was not sampled during initial specimen processing, whether the gross lesion corresponding to the EPC was entirely submitted for histologic evaluation was noted. In addition, the percentage of the specimen submitted for histologic evaluation was estimated by assuming that tissue sections measured 1.6 cm3 (2.0 × 2.0 × 0.4 cm), multiplying 1.6 cm3 by the number of sections submitted, and dividing that number by the total specimen volume, which was calculated from the gross description.
Sentinel lymph nodes were entirely submitted after serial sectioning at 2-mm intervals.
Estrogen receptor (ER) and progesterone receptor (PR) immunostains were reviewed if available, and results were recorded according to standard methods.
Patient data were retrieved from the electronic medical record. Age, type of breast and axillary lymph node surgery, laterality, and outcome, when available, were recorded.
Immunohistochemical Analysis
Formalin-fixed, paraffin-embedded sections were cut at 4 μm. A summary of immunohistochemical materials and methods is given in Table 1. Of note, in addition to standard protease pretreatment, cell conditioning solution 1 (Ventana, Tucson, AZ) was applied to tissue specimens for 30 minutes (mild cell conditioning) before the application of the collagen type IV antibody. This procedure resulted in crisp and intense positive control staining with minimal to no background staining.
View this table:
Table 1
Immunohistochemical Materials and Methods for 27 Cases of Encapsulated Papillary Carcinoma
Immunohistochemical Scoring Method
Smooth muscle–myosin heavy chain (SM-MHC) and p63 were semiquantitatively scored on a scale of 0 to 3+ (0, negative; 1+, focal positive; 2+, patchy, moderate staining; and 3+, intense, patchy to complete staining around lesional epithelium). Laminin and collagen type IV were similarly scored on a scale of 0 to 3+ (0, negative; 1+, focal, weak staining; 2+, patchy, weak to moderate staining or almost complete weak staining with focal areas of discontinuity/absent staining; and 3+, complete, strong, linear staining surrounding 100% of lesional borders).
Results
Histopathologic Features and Hormone Receptor Status
Histopathologic and specimen processing details for 27 patients with EPC (21 without and 6 with invasive carcinoma) are shown in Table 2. Briefly, EPCs ranged in size from 0.5 to 8.0 cm (mean, 2.4 cm; median, 1.7 cm). The mean and median sizes of EPCs without invasion were 2.46 and 1.7 cm, respectively, and the mean and median sizes of EPC with invasion were 2.02 and 1.65 cm, respectively. The majority of EPCs demonstrated the classic features of a distended, expansile duct involved by an epithelial proliferation with a papillary architecture, moderate nuclear grade, and low mitotic index Image 1. The majority were also ER+ (15/18 cases) and PR+ (13/18 cases). Five cases (cases 3, 19, 30, 43, and 66), in contrast with the remaining 22 cases, had grade 3 nuclei and relatively high mitotic rates, ranging from 15 to 60/10 HPF. ER and PR studies were performed in only 2 of these cases (cases 30 and 43), both of which were ER– and PR–.
View this table:
Table 2
Histopathologic and Specimen Handling Details for 27 Cases of EPC
View larger version:
Image 1
(Case 48) Encapsulated papillary carcinoma (EPC) in a patient with stage IV ipsilateral invasive ductal carcinoma 7 years after initial diagnosis. A, EPC with a well-circumscribed border and surrounding sclerosis (H&E, ×20). B, High-power view of the EPC demonstrates classic papillary morphologic features and cytologic atypia (H&E, ×200). C, Ipsilateral invasive ductal carcinoma (IDC) with tubular features occurring 7 years after the diagnosis of EPC (H&E, ×200). D, Synchronous metastasis to the pubic ramus with crush artifact but morphologic features consistent with the primary breast tumor (H&E, ×200). The IDC and metastasis were positive for estrogen receptor.
Six cases of EPC were associated with a synchronous invasive carcinoma (cases 3, 19, 24, 43, 62, and 70). In the latter 5 cases (5/6 [83%]), a single tumor nodule was described grossly that microscopically corresponded to EPC predominantly but with microscopic foci of invasion present adjacent to the EPC or in proximity (<0.5 cm). All of the invasive carcinomas in these cases were of the not otherwise specified type. In only case 3 was a separate tumor nodule seen grossly involving skeletal muscle, which corresponded to an invasive carcinoma separate from the EPC.
Clinical and Outcome Data
Clinical characteristics and outcome data for 27 patients diagnosed with EPC with or without synchronous invasive carcinoma are shown in Table 3.
View this table:
Table 3
Clinical and Outcome Data for 27 Patients With EPC
EPC Without Synchronous Invasive Carcinoma
The average age of the 21 patients in this group was 68.6 years (range, 42–88 years). Of the 21 patients, 14 (67%) underwent segmental mastectomy and 7 (33%) had total mastectomies. Sentinel lymph node biopsies were performed in 11 patients (52%). One patient (case 65) had a micrometastasis in 1 sentinel lymph node, the slides of which were unavailable for review, and did not undergo completion axillary dissection. Immunohistochemical studies were not performed on the lymph node for confirmation of the micrometastases, and the lesion in this case was not entirely submitted for histologic evaluation. The remaining 10 cases were negative for nodal metastases.
Follow-up was available in 13 cases (62%). Follow-up time ranged from 8 to 108 months (mean, 40.4 months). In 1 patient (case 48), ipsilateral IDC and biopsy-proven synchronous bony metastases (pubic ramus) developed 7 years after the initial diagnosis of EPC. The morphologic features of the IDC and bony metastases were distinctly different from that of the EPC (Image 1). All other patients were alive with no evidence of disease.
EPC With Synchronous Invasive Carcinoma
The average age of the 6 patients in this group was 66.3 years (range, 42–80 years). Of the 6 patients, 3 (50%) underwent segmental mastectomy and 3 (50%) had total mastectomies. Axillary node sampling was performed in 5 cases (83%). One patient (case 24) had 2 positive sentinel lymph nodes morphologically similar to the invasive carcinoma. Subsequent axillary dissection was negative.
Follow-up was available in 4 cases (67%). Follow-up time ranged from 4 to 84 months (mean, 28.0 months). In 1 patient (case 3), biopsy-proven supraclavicular lymph node metastases, T11 vertebral bone metastases, and pulmonary metastases developed 3 years, 5 years, and 7 years, respectively, after initial diagnosis of an IDC arising adjacent to an EPC. Material from the supraclavicular nodal and lung metastases were available for review Image 2. Both demonstrated moderate to high-grade ER+ IDC with no papillary morphologic features. Prominent necrosis was also seen in the lung metastases. One additional patient (case 19) had a single hepatic lesion and skull lesions detected by computed tomography and bone scans, respectively, 16 months after the initial diagnosis of IDC and EPC that were suggestive of malignancy but were not biopsied. The remaining 2 patients with clinical follow-up were alive with no evidence of disease.
View larger version:
Image 2
(Case 3) Encapsulated papillary carcinoma (EPC) and synchronous invasive ductal carcinoma in a patient with distant metastases. A, EPC with a well-circumscribed border and central hemorrhage (H&E, ×20). B, Higher-power view of the EPC demonstrates high-grade ductal epithelium lining a fibrovascular core (H&E, ×400). C, An invasive ductal carcinoma, not otherwise specified, was present in the adjacent breast. D and E, At 3 and 7 years after initial diagnosis, supraclavicular (D, H&E, ×400) and lung (E, H&E, ×400) metastases developed, respectively. Note the metastases show no papillary morphologic features and are histologically akin to the primary invasive ductal carcinoma shown in C.
Immunohistochemical Results
Data for p63, SM-MHC, and collagen type IV are shown in Figure 1, Figure 2, and Figure 3, respectively. As expected, all papillomas showed positive immunoreactivity at their periphery with both myoepithelial markers, and all but one case showed 3+ staining for collagen type IV Image 3. DCIS demonstrated identical results for collagen type IV; however, 3 cases, all of which had papillary morphologic features, were negative for p63 and SM-MHC despite positive internal controls Image 4. All SPCs were negative for p63, and the majority were negative or showed 1+ staining for SM-MHC. Collagen type IV results in SPCs were more variable, although the majority showed 2+ or 3+ staining. All cases of IDC were negative for myoepithelial markers, and the majority were negative or 1+ for collagen type IV. It is interesting that 3 cases showed 2+ collagen type IV results represented by near-complete, linear staining around nests of tumor cells but with foci of discontinuity or fragmentation Image 5.
View larger version:
Figure 1
Immunohistochemical data for p63 staining in papilloma, ductal carcinoma in situ (DCIS), encapsulated papillary carcinoma (EPC), solid papillary carcinoma (SPC), and invasive ductal carcinoma (IDC). Semiquantitative scoring was as follows: 0, negative; 1+, focal positive; 2+, patchy, moderate staining; and 3+, intense, patchy to complete staining around lesional epithelium.
View larger version:
Figure 2
Immunohistochemical data for smooth muscle-myosin heavy chain staining in papilloma, ductal carcinoma in situ (DCIS), encapsulated papillary carcinoma (EPC), solid papillary carcinoma (SPC), and invasive ductal carcinoma (IDC). Semiquantitative scoring was as follows: 0, negative; 1+, focal positive; 2+, patchy, moderate staining; and 3+, intense, patchy to complete staining around lesional epithelium.
View larger version:
Figure 3
Immunohistochemical data for collagen type IV staining in papilloma, ductal carcinoma in situ (DCIS), encapsulated papillary carcinoma (EPC), solid papillary carcinoma (SPC), and invasive ductal carcinoma (IDC). Scoring was as follows: 0, negative; 1+, focal, weak staining; 2+, patchy, weak to moderate staining or almost complete weak staining with focal areas of discontinuity or absent staining; and 3+, complete, strong, linear staining surrounding 100% of lesional borders.
View larger version:
Image 3
Collagen type IV expression in a benign papilloma. A, An intracystic, benign papilloma (H&E, ×40). B, Collagen type IV completely surrounds the perimeter of the papilloma and additionally highlights its fibrovascular cores (×40). C, Intense, linear and continuous collagen type IV staining at the periphery of the papilloma (×200).
View larger version:
Image 4
Collagen type IV expression in ductal carcinoma in situ (DCIS). A, Cribriform DCIS (H&E, ×100). B, Myoepithelial cell marker smooth muscle–myosin heavy chain demonstrates linear, intense staining at the periphery of the ducts (×100). As expected, p63 showed similar results (not shown). C, Similar to the myoepithelial markers, collagen type IV expression was seen as intense, linear staining around ducts (×100). D, Papillary DCIS with necrosis (H&E, ×100). E, Myoepithelial cell markers, such as p63 depicted here, were unexpectedly negative in a subset of DCIS cases that had predominantly papillary morphologic features (×100). F, In contrast with the myoepithelial cell markers in this case, intense, linear and complete collagen type IV expression was seen at the periphery of the duct (×100).
View larger version:
Image 5
Collagen type IV expression in invasive ductal carcinomas. A, Invasive ductal carcinoma, not otherwise specified (NOS) (H&E, ×200). B, Collagen type IV deposition was absent or significantly decreased in the majority of invasive carcinomas and highlights only capillaries and adipocytes (×400). C, Invasive ductal carcinoma, NOS (H&E, ×200). D, A subset of the invasive carcinomas demonstrated 2+ collagen type IV expression, as seen here, represented by linear but discontinuous staining (×200).
Raw data for immunohistochemical results in EPCs are shown in Table 4. The majority of EPCs were negative for both myoepithelial markers; however, collagen type IV showed 3+ immunoreactivity in the majority of cases (17/26 [65%]) and 2+ immunoreactivity in the remaining 9 cases (35%) Image 6. In examination of cases of EPC with an adjacent IDC (cases 3, 19, 24, 43, 62, and 70), 4 of the 6 cases showed 2+ collagen type IV staining, with patterns of continuous intense staining around the majority of the EPC with foci of weaker staining and discontinuity often seen adjacent to the IDC Image 7.
View this table:
Table 4
Immunohistochemical Results in 27 EPCs
View larger version:
Image 6
Collagen type IV expression in encapsulated papillary carcinomas (EPCs). A-D (Case 66), A, The periphery of a classic EPC (H&E, ×40). B, p63, in addition to myoepithelial marker smooth muscle–myosin heavy chain, was negative in the majority of EPCs (p63, ×40). C and D, In contrast, complete (3+) collagen type IV expression was present in the majority of EPCs (C, ×20; D, ×100). E-H (Case 30), E and F, Some EPCs demonstrated high-grade nuclear morphologic features (E, H&E, ×20; F, H&E, ×400). G and H, Collagen type IV expression more often showed 2+ expression in EPCs with high-grade morphologic features, represented by foci of continuous staining but other areas of weak and/or discontinuous expression (G, ×20; H, ×200).
View larger version:
Image 7
(Case 62) Collagen type IV immunohistochemical staining in an encapsulated papillary carcinoma (EPC) with adjacent invasive ductal carcinoma. A, Low-power view of a well-circumscribed EPC with a frank adjacent invasive carcinoma (H&E, ×40). B and C, Collagen type IV expression was seen in a continuous manner in parts of the EPC (B, ×20) and showed fragmentation, particularly adjacent to the invasive carcinoma (C, ×100). D, The adjacent invasive carcinoma was negative for collagen type IV. Note the intense perivascular staining (collagen IV, ×200).
Collagen type IV was uniformly expressed in a continuous manner around benign ducts and lobules. It also showed intense, linear perivascular and adipocyte staining and was noted to be relatively increased in the stroma of sclerosing adenosis.
Immunohistochemical analysis with the laminin antibody was attempted in the first 25 cases (including papillomas, DCIS, EPC, and IDC) included in the study (data not shown). The results were extremely variable and difficult to interpret, and we elected to discontinue its study.
Discussion
Although EPCs have been traditionally considered to be a variant of DCIS, recent studies demonstrating a lack of myoepithelial cell markers at their periphery suggest otherwise. However, the present study demonstrated continuous, intense collagen type IV immunoreactivity entirely circumscribing the majority of these lesions, highly suggestive that EPCs are confined within an intact basement membrane and are thus in situ carcinomas. In support of this conclusion, all patients in our study with “pure” EPC (no synchronous or adjacent invasive carcinoma) in whom axillary lymph node sampling was performed were node-negative, except for 1 case that showed micrometastasis. In this case, the lymph node slides were not available for review, and, moreover, the lesion was not entirely submitted for histologic evaluation. Therefore, the possibility of an occult invasive carcinoma cannot be entirely excluded. Apart from this 1 case, these results parallel previous reports of more than 50 cases of EPC with negative axillary nodes.2,12–14 In addition, they parallel reported outcome data indicating that EPCs have an excellent prognosis with adequate local therapy alone.2,12–15
As previously mentioned and in contradiction to this finding, several studies have reported cases of EPC with metastases. In one of these reports, lung metastases developed in 1 of 21 patients, and all others were alive with no evidence of disease, although specimen processing or whether the entire EPC or specimen was submitted for microscopic examination was not described.2 In a second report, 2 patients with pure EPC and micrometastases to axillary lymph nodes were described.6 In the first case, the tumor in the lumpectomy specimen was entirely submitted for microscopic examination, yet the micrometastasis depicted in this report does not have papillary architecture. The specimen from the second patient with nodal micrometastases was described as “extensively sampled,” and it is thus unclear whether the entire EPC, or at least its border, was submitted. Similarly, a third study that reported metastases in 3 (4%) of 77 patients with EPC did not entirely submit the lesion of interest.15 In our current data set, 6 (22%) of 27 EPCs were associated with an IDC, and of these, 4 (67%) were entirely submitted for histologic examination (Table 2). Furthermore, a single lesion was described grossly in 5 cases (83%), which corresponded predominantly to EPC but with foci of adjacent IDC, not otherwise specified, noted on microscopic examination. It is thus imperative to extensively sample these lesions to rule out an adjacent invasive carcinoma, and we recommend submitting them entirely to do so.
Although immunohistochemical detection of the basement membrane can be challenging, we have developed a robust method that provides for accurate interpretation for the presence of type IV collagen. The pattern of collagen type IV expression seen in benign and in situ lesions studied was that of an intense, continuous linear pattern around involved ducts, which was seen in the majority of EPCs. In contrast, the majority of IDCs were negative or showed focal collagen type IV expression. However, 3 cases of IDC (30%) and 9 cases of EPC (35%) showed 2+ collagen type IV expression as represented in Images 5 and 6, respectively. It has been previously shown that some clearly invasive neoplasms display a continuous basement membrane, particularly well-differentiated, low-grade tumors such as cutaneous well-differentiated squamous cell carcinomas and basal cell carcinomas.16,17 Thus, it may be argued that our finding of a continuous basement membrane around EPC does not definitively prove that they are in situ lesions but instead supports the hypothesis that they are low-grade invasive neoplasms. Basement membrane studies of the breast, however, have consistently shown type IV collagen expression in a continuous manner in benign and in situ lesions and absent or fragmented-discontinuous expression in invasive carcinomas, including tubular carcinomas.11,18–21 Indeed, the interpretation of basement membrane immunostains is crucial in differentiating in situ from invasive carcinomas: complete and continuous expression is seen in benign and in situ lesions and absent or fragmented-discontinuous expression is seen in invasive carcinomas. Based on our data, EPCs are thus in situ carcinomas.
The majority of EPCs in our study demonstrated a moderate degree of nuclear pleomorphism and were ER+ tumors with a low mitotic index. Five cases instead showed high-grade nuclei and mitotic indexes of 15 to 60/10 HPF. Two of these had been previously tested for hormone receptors, both of which were negative. It is interesting that 4 of the 5 cases displayed 2+ collagen type IV staining and 3 of the 5 were associated with invasive carcinoma. In a previous study that visualized the basal lamina using digital color image processing, a continuous basal lamina was present around the glands in 33 of 39 DCIS cases but was absent or discontinuous in the remaining 6 cases, all of which were high-grade DCIS with necrosis.20 Also, in a study of 77 EPCs, patients with higher-grade tumors had an increased risk of recurrence and metastasis.15 Such findings suggest that decreased collagen type IV expression is a manifestation of an in situ carcinoma “in transition” to an invasive neoplasm with concomitant loss of the basement membrane.
EPCs ranged in size from 0.5 to 8.0 cm (Table 2). However, the tumor size in 4 cases in which the gross measurement was more than 5.0 cm (cases 30, 39, 65, and 68) was likely overestimated based on retrospective review of the gross pathology report and histologic slides. In case 30, there was extensive DCIS adjacent to the EPC. In cases 39 and 65, the tumor size was based on measurement of the biopsy cavity in the mastectomy specimen, and in case 68 a previously biopsied cyst with brown fluid was described grossly. It is likely that adjacent DCIS and/or prior biopsy may cause overestimation of the size of EPCs, especially given the tendency of these lesions to hemorrhage and become necrotic after biopsy.
An unexpected finding was the absence of myoepithelial cell markers at the periphery of 3 cases of papillary DCIS (Image 4). All, however, were surrounded by continuous, intense collagen type IV. They thus may represent “early” EPCs or EPCs extending into smaller ducts. This finding solicits the question of why myoepithelial cells are absent in EPCs and in such apparent DCIS cases with papillary morphologic features. Some authors have suggested that myoepithelial cells become attenuated or altered owing to their compression by the expansile growth of EPCs.4 This hypothesis does not account for our finding of apparent papillary DCIS with absent myoepithelial cell markers. An alternative explanation is that these papillary lesions exert a paracrine effect on adjacent myoepithelial cells resulting in dissolution or alteration of proteins commonly used to detect them immunohistochemically (such as p63 and SM-MHC). Such a phenomenon, however, is not necessarily restricted to DCIS with papillary morphologic features because myoepithelial cells can be variably present at the periphery of solid DCIS as well.22
EPCs of the breast usually manifest in postmenopausal women. They are typically low-grade neoplasms with absent myoepithelial cells at their periphery but show a continuous envelopment of basement membrane as demonstrated by immunohistochemical detection of collagen type IV and are thus best considered in situ carcinomas. Apparent EPCs with high-grade nuclear morphologic features and high mitotic indexes are more often associated with an invasive component and may in fact be in situ carcinomas in transition to invasive carcinomas based on the collagen type IV data presented. Similar to high-grade, palpable DCIS, in which sentinel lymph node biopsies are generally recommended given reported positive sentinel lymph node rates of approximately 13%,23,24 sentinel lymph node biopsies may be considered after a diagnosis of EPC on biopsy. Finally, an invasive component should be excluded by entirely submitting the borders of the EPC given the possibility of an associated occult, invasive carcinoma.
Acknowledgments
We thank Kimberly McManus for her expertise and involvement in the optimization of the collagen type IV immunohistochemical procedure.












{kind=link}