



























| 图片: | |
|---|---|
| 名称: | |
| 描述: | |
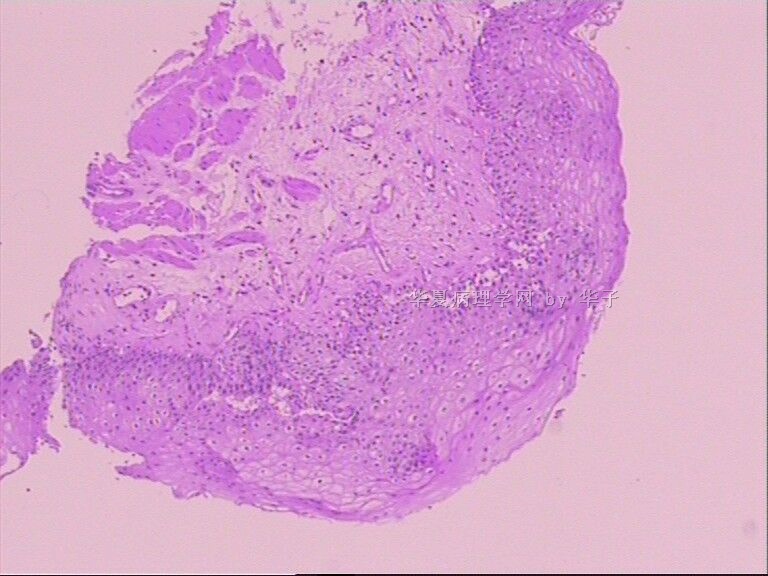
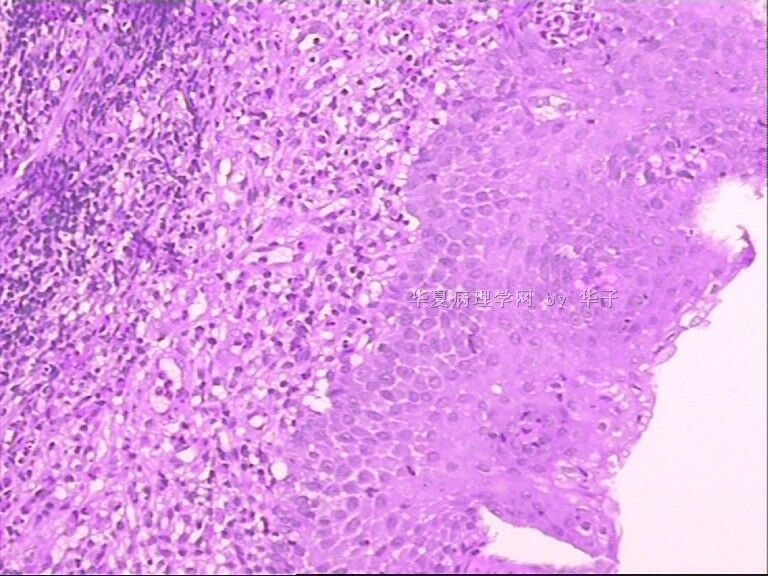
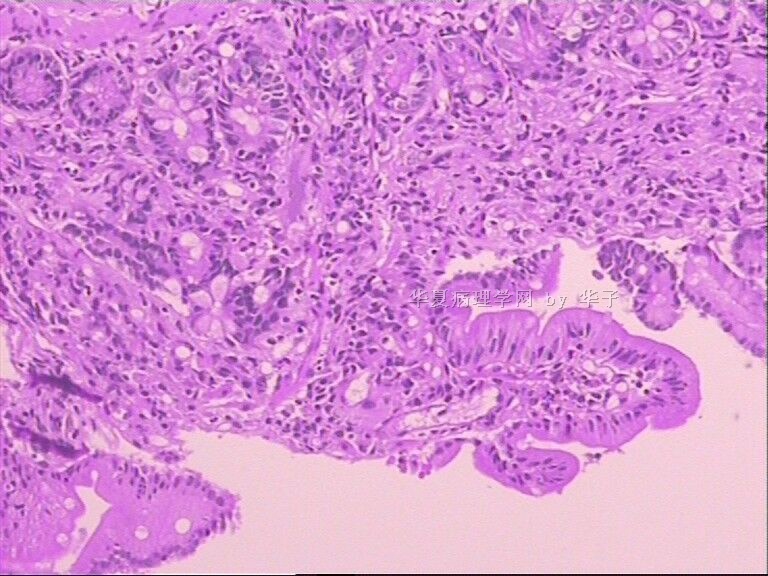
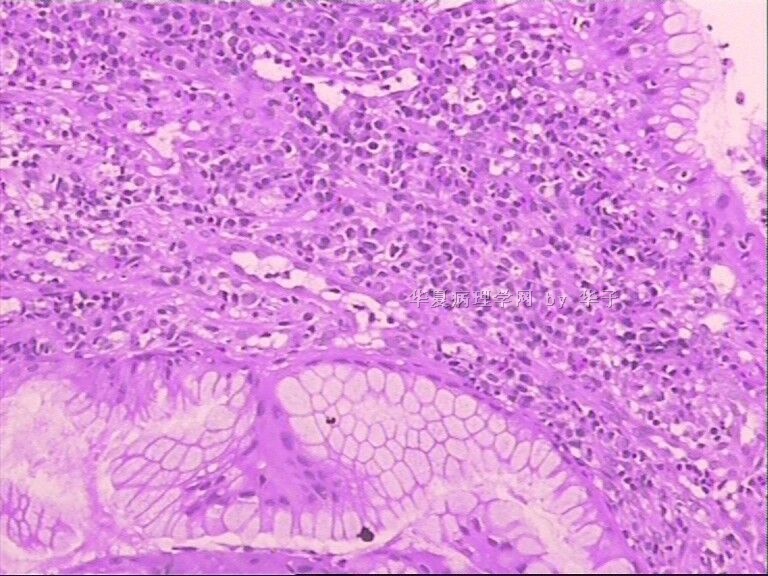
- 儿童胃粘膜活检-罕见病变
| 以下是引用海上明月在2010-7-2 18:10:00的发言:
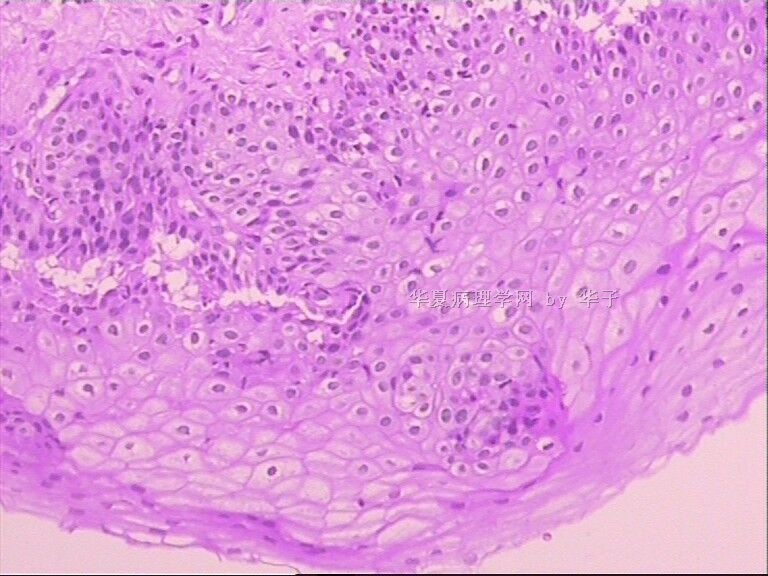
非常赞成先天性粘膜异位+炎症性改变。 正常发育的胃粘膜无论如何会见到胃腺,可是本例胃体和胃底部取材根本见不到胃固有腺体-胃底腺,而所见的是复层上皮既不像完全的鳞状上皮,也不像肠上皮,处于胎儿时期食管-胃连接处处于发育但尚未达到完全成熟的伴有杯状细胞的复层上皮(食管远端粘膜异位?),又很像假复层纤毛柱状上皮被部分鳞化,不仅可见杯状细胞,还偶见纤毛柱状上皮,所以推测很有可能是气管粘膜异位。 异位的粘膜由于缺乏胃底腺,不适宜于进入胃内的食物初步消化成食糜的功能,在半岁-1岁时期,奶汁等流质饮食为主,使胃内容物容易排空,不至于引发炎症。到了3岁,可能以常规食物为主,这个胃就不能适应了,由于胃初步消化和排空功能受到影响,长此便引发严重的炎症反应。 按照这样的推测,该3岁患儿以前可能显示有上腹部不适伴有消化不良逐渐加重的症状。建议补充病史。 以上纯属推测,谬论难免,请指正。谢谢! 仅供参考! |
| 以下是引用njlihua在2010-6-28 17:31:00的发言:
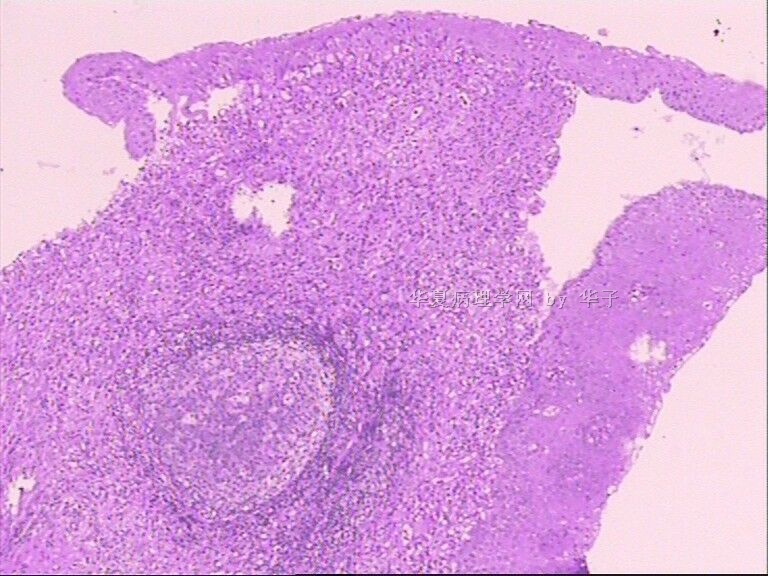
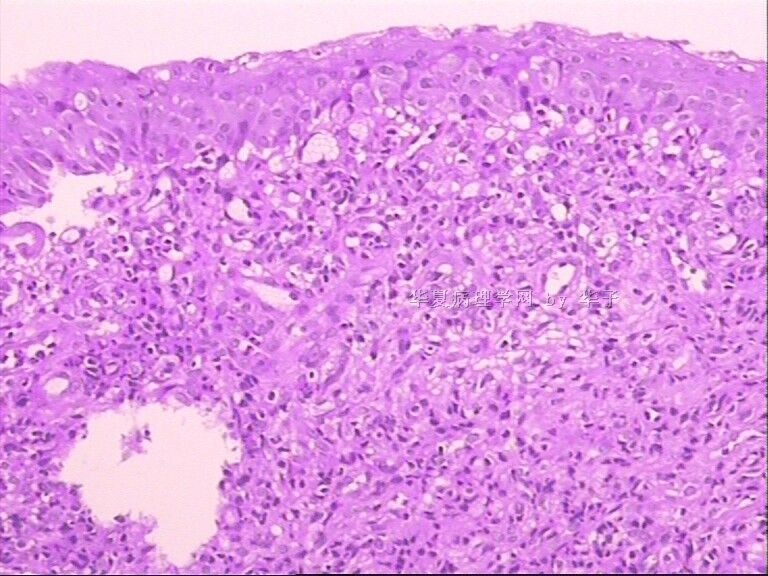
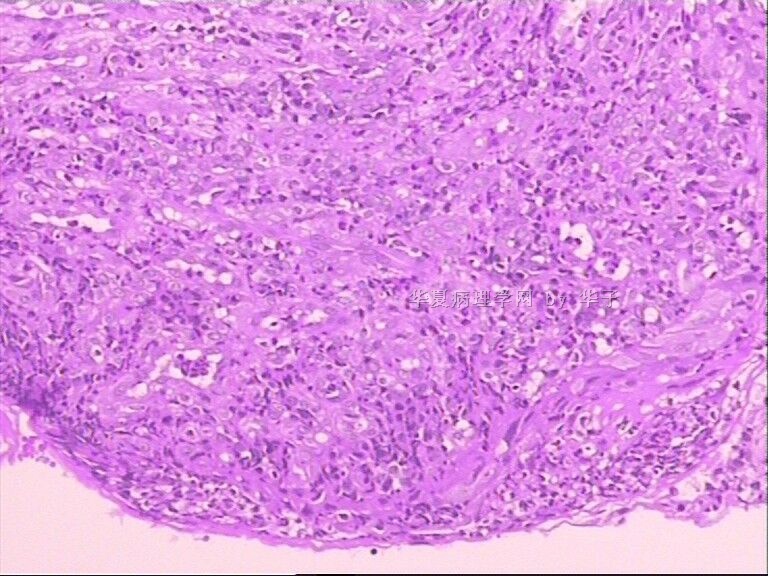
这个病例很有意思,但总体印象不太像恶性。 整个片子中固有层内炎症细胞浸润明显,包括淋巴细胞,浆细胞和中性粒细胞,腺体间距增宽,可见类似肠道的隐窝脓肿,表面上皮明显增生,粘液分泌旺盛,我个人认为那种细胞不一定是杯状细胞,就像在Barrett食管时,分泌粘液的细胞有时形态类似杯状细胞,应该做AB PH2.5的染色。 仔细观察有无HP感染,如有是否为HP感染引起的胃炎; 请临床观察有无肠道病变,需要排除炎症性肠病,有时炎症性肠病可以出现上消化道异常,最常见是crohn病,仔细寻找有无上皮样肉芽肿。 最后考虑全身疾病累及胃或其他特殊病变,就不是十分清楚了。 |
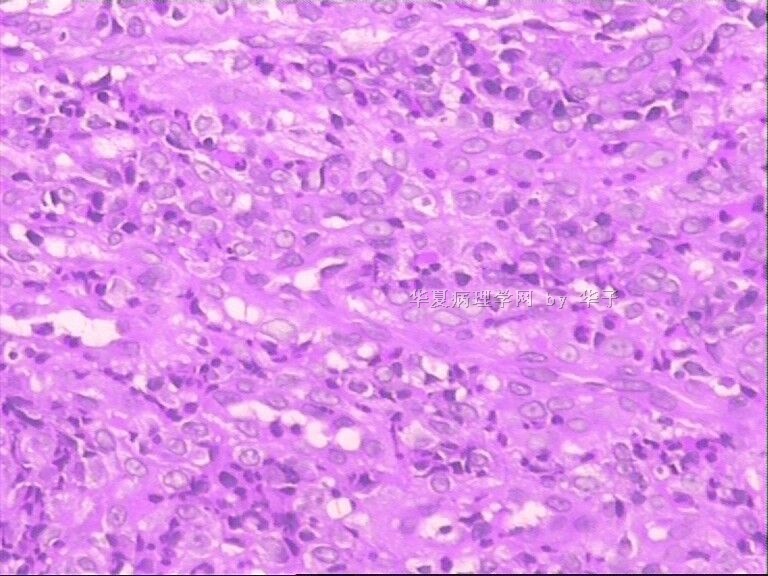
It looks like an inflammatory lesion with plasma cells, lymphocytes, histiocytes, neutrophils and eosinophils. I don't think it is neoplastic although there are intraepithelial inflammatory cells, they do not appear to be particularly destructive. I favor an autoimmune or allergic process than an infectious process, among others. I had trouble reading many of the slides off the terminal. Is the structure being highlighted on the fourth row on the right a multinucleated giant cell or are those multiple individual cells? What were the endoscopic findings? I suspect it was diffuse erythema and hemorrhage with no mass lesions. Any lower GI symptoms?
I like the suggestions made by 第 19 楼: "非常需要了解临床具体情况:如有无感染、过敏、用药、胆汁返流、炎性肠病等情况."
It looked like the PAS stain did not highlight microorganisms. If it is neoplastic (again unlikely) a T-cell process would be at the top of my list.
 | |
|
|
-
本帖最后由 于 2010-07-03 10:52:00 编辑
全胃粘膜发育异常,看来还是与遗传缺陷有关,这是一个值得遗传病理学研究的病例。请见另一处的介绍:
| 以下是引用华子在2010-7-2 20:05:00的发言:
倒数第5张是十二指肠正常粘膜,内镜显示食道及十二指肠未见明显病变。倒数第二张是AB-PAS显示上皮表面似为纤毛的染色效果,不是细菌。 该家庭中五个小孩,三个女孩都正常,第一个男孩因腹泻病死亡,这是第二个男孩。 |

- 王军臣
-
angyang303 离线
- 帖子:79
- 粉蓝豆:15
- 经验:105
- 注册时间:2009-05-21
- 加关注 | 发消息
-
本帖最后由 于 2010-07-05 10:18:00 编辑
| 以下是引用谈东风在2010-7-5 0:15:00的发言:
谈教授说: 上述该家族史很重要!! 需要了解那个亡故男孩更加详实的病史资料。他是多大年龄时去世的?有什么临床表现?腹泻多长时间?做过胃肠道活检吗?病理变化如何? |
- 王军臣
| 以下是引用海上明月在2010-7-3 10:51:00的发言:
全胃粘膜发育异常,看来还是与遗传缺陷有关,这是一个值得遗传病理学研究的病例。请见另一处的介绍:
That's a very important family history!!
We need more detailed information about the death of that boy? At what age did he die? what was his clinical presentation? how long was his diarrhea? Any GI biopsy was done? What was the pathological changes?
Thanks. |
-
本帖最后由 于 2010-07-05 20:39:00 编辑
非常具有挑战性的病例。就家族史分析, 其兄死于“腹泻”,而患儿为4个月的“呕吐”。临床表现显然不同,但其共性为胃肠道运动障碍“Motility Disorders”。如能除外因感染和自身免疫等因素引起胃粘膜固有腺体的严重损伤,那有可能因长期严重反流造成的胃粘膜损伤"表象"。而其"本质"是运动障碍。Motility Disorders 可分为“GI神经疾病”和“GI肌肉疾病”。粘膜活检表浅,病理学是无法观察的粘膜下/肌间神经丛和Cajal细胞。
- xljin8
| 以下是引用谈东风在2010-7-5 0:15:00的发言:
 |
| 以下是引用华子在2010-6-26 21:19:00的发言:
|
Pathologically, pseudogoblet cells are typically arranged in discrete rows and clusters, often in the uperficial parts of the epithelium, whereas goblet cells typically occur as single cells or distributed randomly within the metaplastic columnar epithelium.
unfortunately, no immunohistochemical or mucin histo chemical stains, including alcian blue, can
reliably distinguish true goblet cells from pseudogoblet cells. although goblet cells are typically alcian-bluepositive (at pH 2.5, which indicates the presence of acidic mucins), pseudogoblet cells usually reveal weak posi tivitywith this stain at this pH level as well. Furthermore, nondistended, mucinous, columnar cells of normal appearance also typically stain positive with alcian blue, even those from the proximal stomach.
Thus, in my opinion, alcian blue cannot be reliably used to confirm the presence of metaplastic columnar epithelium or to distinguish true goblet from pseudogoblet cells in biopsy specimens from the distal esophagus or gastroesophageal junction.
- 境随心转











