














 学习一下。
学习一下。 | 图片: | |
|---|---|
| 名称: | |
| 描述: | |
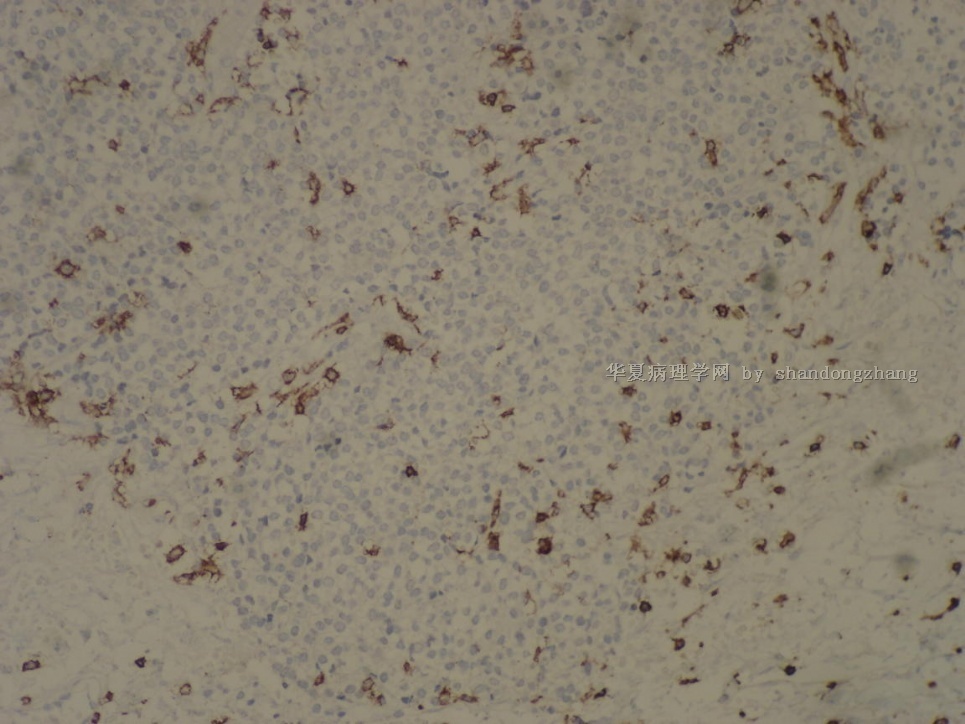
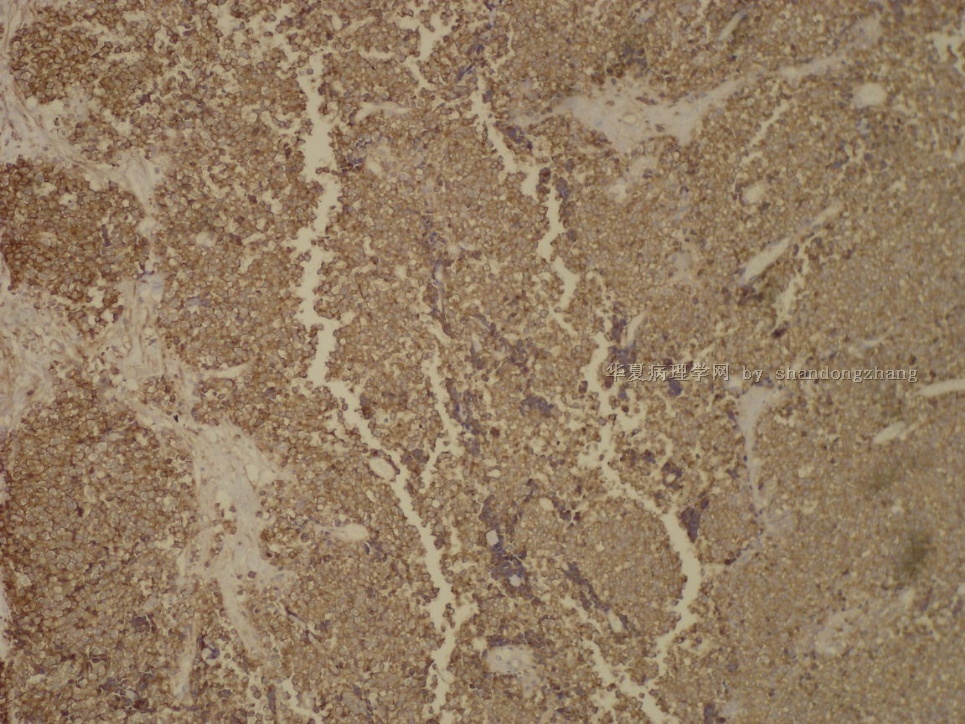
- 20100126-输尿管肿物
-
本帖最后由 于 2010-01-27 21:29:00 编辑
*The characteristic immunohistochemical profile including vimentin, CD99 , and FLI-1, with variable immunohistochemical reactivity for neural markers.
*Immunohistochemistry can be used to distinguish ES/PNET from RMS, and other small blue cell tumor mimics, with the recognotion of the neither CD99 nor FLI-1 are completely specific for ES/PNET in this context and that a diagnostic panel of immunohistochemical stains is necessary.
此二段是摘自Diagnostic Immunohistochemistry, 2nd Edition,p621,2006.
实际上部分RMS(横纹肌肉瘤)可以表达CD99 和 FLI-1。因此,要排除RMS必须肌源性标记阴性。

- xljin8
Mod Pathol. 2004 May;17(5):547-52.
Utility of the immunohistochemical detection of FLI-1 expression in round cell and vascular neoplasm using a monoclonal antibody.
Rossi S, Orvieto E, Furlanetto A, Laurino L, Ninfo V, Dei Tos AP.
Department of Pathology, Regional Hospital, Treviso, Italy.
FLI-1 nuclear transcription factor has been proposed as a useful tool in the differential diagnosis of small round cell sarcomas. Recently, FLI-1 has been reported as the first nuclear marker of endothelial differentiation. However, its clinical use has been hampered by major interpretation problems, due to the presence of background staining as well as staining variation between different lots of the same antiserum. In this study, a novel monoclonal antibody raised against the carboxyl terminal of the FLI-1 protein (clone GI146-222, BD Pharmingen) was tested in a series of small round cell and vascular neoplasms. Furthermore, in order to assess FLI-1 specificity, we analyzed its expression in a series of common epithelial and nonepithelial malignancies. In total, 15 Ewing's sarcomas, 10 rhabdomyosarcomas, 5 desmoplastic small round cell tumors, 10 synovial sarcomas, 10 high-grade pleomorphic sarcomas, 10 malignant melanomas, 5 Merkel's carcinomas, 10 colonic adenocarcinomas, 10 breast carcinomas, 10 lung adenocarcinomas, 20 angiosarcomas, 5 epithelioid hemangioendotheliomas, 10 Kaposi's sarcomas and 10 benign hemangiomas, were stained. A strong FLI-1 immunoreactivity was detected in all Ewing's sarcomas and vascular neoplasms, highlighting the high sensitivity of FLI-1 monoclonal antibody. However, 2/5 Merkel's carcinomas and 1/10 malignant melanomas showed a strong nuclear immunostaining, suggesting that FLI-1 may not be so helpful in the differential diagnosis of cutaneous Ewing's sarcoma. In addition, a weak immunoreactivity was found in 3/5 Merkel cell carcinomas, 3/10 synovial sarcomas, 5/10 malignant melanomas, 6/10 lung adenocarcinomas and in 1/10 breast carcinomas. In contrast, all the rhabdomyosarcomas, desmoplastic small round cell tumors, high-grade pleomorphic sarcomas and colonic adenocarcinomas tested were negative. Importantly, in contrast with previous studies, no background staining was observed. Our results indicate that FLI-1 monoclonal antibody can be reliably applied to the differential diagnosis of small round cell neoplasms of soft tissue, and confirm its important role as nuclear marker of endothelial differentiation, mainly helpful in those cases in which technical artifacts are seen by using the traditional membranous and cytoplasmic endothelial markers.
- 王军臣
-
本帖最后由 于 2010-01-28 01:34:00 编辑
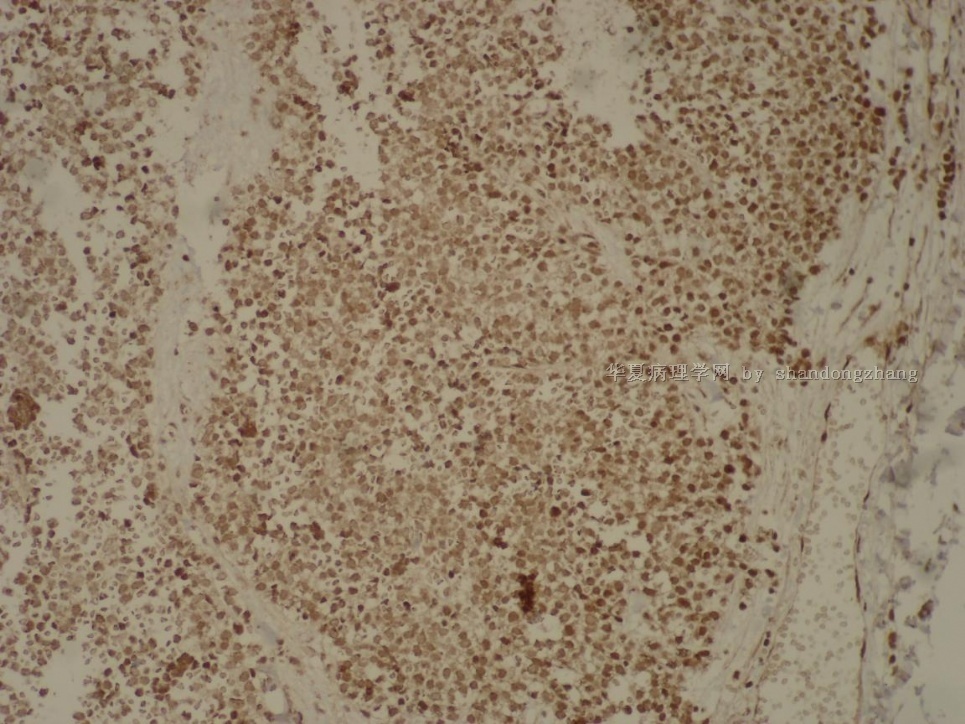
| 以下是引用96298在2010-1-27 20:33:00的发言: 支持:Ewing's sarcomas / PNET,除外横肉。 问题 Fli-1 是什么? |
请见上述文献。Fli-1是一种核转录因子,当ES/PNET有t(11; 22)(q24;q12) 基因易位时,引起EWS 与 FLI-1基因融合(EWS-FLI-1融合基因),导致 FLI-1蛋白高表达。使用Fli-1单克隆抗体作免疫组织化染色,可显示该蛋白的表达。由于是核转录因子,所以阳性定位在核内。
- 王军臣
Am J Surg Pathol. 2000 Dec;24(12):1657-62.
Immunohistochemical detection of FLI-1 protein expression: a study of 132 round cell tumors with emphasis on CD99-positive mimics of Ewing's sarcoma/primitive neuroectodermal tumor.
Folpe AL, Hill CE, Parham DM, O'Shea PA, Weiss SW.
Department of Pathology and Laboratory Medicine, Emory University, Atlanta, Georgia, USA. afolpe@emory.edu
The histologic and immunohistochemical differentiation of Ewing' s sarcoma/primitive neuroectodermal tumor (ES/PNET) from other small, blue, round cell tumors may be difficult. Despite initial promise, CD99 (MIC2) has not proven to be a specific marker. Approximately 90% of ES/PNET have a specific t(11; 22)(q24;q12) that results in fusion of the EWS and FLI-1 genes, and overexpression of FLI-1 protein. A recent study has shown immunohistochemical FLI-1 expression in five of seven of the ES/PNET cases tested. We evaluated FLI-1 expression in 132 well-characterized small, blue, round cell tumors. All tumors were immunostained for FLI-1 (1:40, Sc 356 polyclonal, Santa Cruz Biotechnology) using steam heat for epitope retrieval. Only nuclear staining was accepted as positive. Endothelial cells were strongly positive in all cases and served as an internal control. In many cases, a subset of lymphocytes also stained positive. No staining was seen in any other normal tissue. FLI-1 expression was seen in 29 of 41 (71%) ES/PNET, 7 of 8 (88%) lymphoblastic lymphomas, 0 of 8 poorly differentiated synovial sarcomas (PDSS), 0 of 32 rhabdomyosarcoma (RMS), 0 of 30 neuroblastomas, 0 of 8 esthesioneuroblastomas, 0 of 3 Wilms' tumors, 0 of 1 mesenchymal chondrosarcoma, and in 1 of 1 desmoplastic round cell tumor. This last case was known to have an EWS/WT-1 fusion. Although the EWS/FLI-1 fusion gene is specific for ES/PNET, FLI-1 protein expression is not. Significantly, the great majority of lymphoblastic lymphomas (also CD99-positive) are strongly FLI-1-positive. Immunohistochemical detection of FLI-1 may be valuable in confirming the diagnosis of ES/ PNET in cases in which molecular genetic evaluation is not feasible. FLI-1 protein expression is also helpful in distinguishing ES/PNET from other tumors that may be CD99-positive, such as PDSS and RMS. It is not surprising that some ES/ PNET are FLI-1-negative, because not all ES/PNET have the classic EWS/FLI-1, and some cases of ES/PNET may produce either low levels of protein or idiotypically different protein.
- 王军臣
-
本帖最后由 于 2010-01-28 03:21:00 编辑
| 以下是引用xljin8在2010-1-28 3:14:00的发言:
有关FLI-1 特异性的IHC研究 Friend
leukaemia integration-1 expression in malignant and benign tumours: a multiple
tumour tissue microarray analysis using polyclonal antibody. BACKGROUND:
Friend leukaemia integration-1 (FLI-1) antibody is a useful marker by
immunohistochemical analysis on 4323 tumours using multiple tumour microarrays,
as well as on whole sections. RESULTS: FLI-1 was expressed in 46/62 EWS/PNETs,
2/3 olfactory neuroblastomas, 7/102 small cell carcinomas of the lung,10/34
MCCs, 1/14 rhabdomyosarcoma, 19/132 non-Hodgkin's lymphomas, 2/3 DSRCTs,and in
53/74 benign and malignant vascular tumours. In addition, 27/508 squamous cell
carcinomas, 19/837 adenocarcinomas, 10/400 urothelial bladder cancers, 1/40 basal
cell carcinomas, 3/29 liposarcomas, 1/40 glioblastoma multiforme and 9/29 medullar
carcinomas of the breast expressed FLI-1. The sensitivity and specificity of
FLI-1 to distinguish EWS/PNET from all types of malignancies were 74.2% and
96.0%, respectively. Finally, the sensitivity and specificity of FLI-1 to
distinguish EWS/PNET from other small round cell tumours (SRCTs) were 74.2% and
91.6%, respectively. CONCLUSION: This study was the first to show that FLI-1 can
be seen in a variety of solid tumours, some of which had never been explored before.
This finding should be kept in mind, especially when using FLI-1 as a marker
for finding the primary origin of poorly differentiated metastatic tumour. |
- xljin8











