









| 图片: | |
|---|---|
| 名称: | |
| 描述: | |
- Parotid FNA
-
翻译一下陈老师的点评:
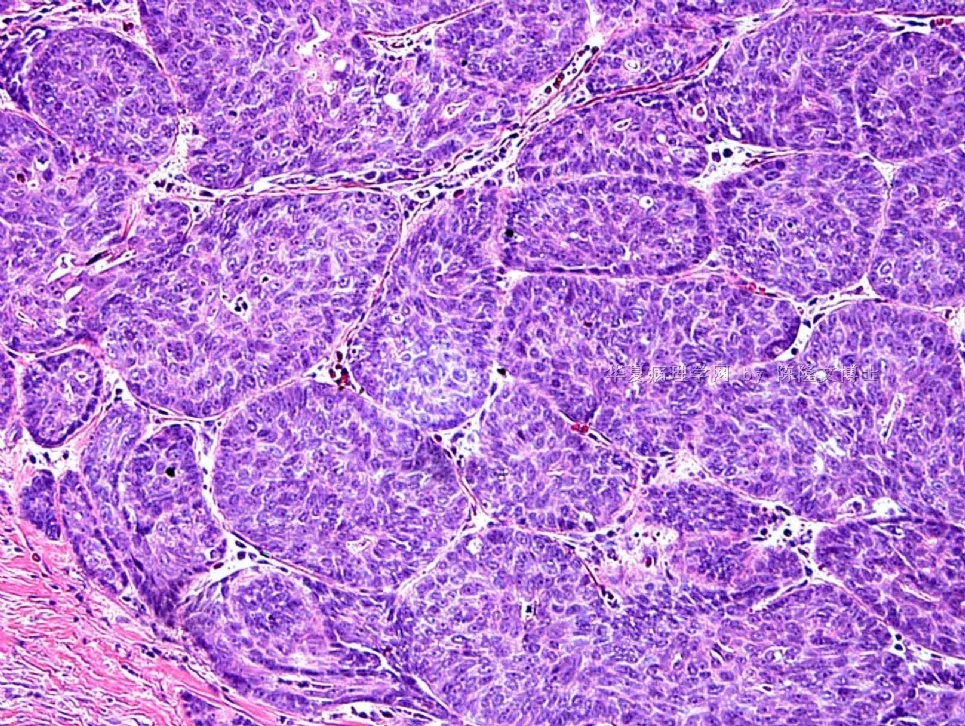
谢谢大家的讨论。Urbio:你讲的蛮不错。本例的最后的病理诊断是基底细胞腺癌。我放了3张最后的HE染色的照片,第一张清楚地显示肿瘤浸润到肌组织,第三张显示坏死和增多的分裂相。
我发的细胞学的诊断是:来源于低级别涎腺上皮/肌上皮肿瘤的不典型细胞。我们的头颈外科大夫见到这个诊断后很清楚该怎么做(外科切除)。因为大多数涎腺原发肿瘤都需要切除。你犯不着讲一个错误的细胞学诊断而使自己难堪。在涎腺的细针穿刺中,如果没得到典型的细胞学特征的话,还是推荐使用笼统些的诊断用语。反过来讲,如果细胞学特征对某肿瘤非常特异,我的诊断也会非常明确。
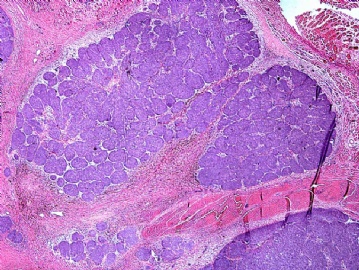 图1
图1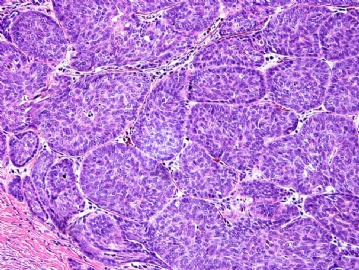 图2
图2 图3
图3
Thank you for all the discussion. Urbino: your comments are well-done. The final pathology for this case is Basal cell adenocarcinoma, I put 3 photos of the final H&E, the first one clearly show the invasion of the muscle, the third one shows necrosis and increased mitoses.
This case the cytology is signed out by me as "atypical cells derived from a low-grade salivary gland epithelial/myoepithelial neoplasm", using this terminology, our Head&Neck surgeons know exactly what to do (surgical excision). Because most of the primary salivary gland tumors need to be removed anyway. You don't need to say wrong diagnosis on cytology to make yourself look bad. A general terminology is recommended in salivary gland FNA when the cytology is NOT typical of a specific neoplasm. On the other hand, if the cytology is perfect for a specific neoplasm, I will say so in the diagnosis.
| 以下是引用陈隆文博士在2009-10-24 0:03:00的发言: I think that people are in the right direction. I have said this many times here that if a salivary gland tumor lacks chondroid-myxoid stroma, I would not call this "pleomorphic adenoma" (PA) on cytology, even if by statistics, it might well be PA, thoes so called "cellular pleomorphic adenoma". I have the surgical resection of this tumor and it again teaches me that the category of the epithelial/myoepithelial tumor of the salivary gland includes a broad differential diagnosis. Anyone want to guess what the final pathology will be? |
这个肿瘤良性的可能性大。不是基底细胞腺瘤就是多形性腺瘤。
也有难说的,毕竟穿刺针路经的区域有限。
顺便提一个建议,想请陈博士尽可能用中文表述。这样,广大基层网友可能阅读起来更加便捷,更加欢迎。如有不便,那就劳驾翻译团队了。谢谢!

- 王军臣
-
OK! 在陈老师的鼓励下,我大胆提几个!
本例的背景无粘液,细胞形态温和,形态单一,核浆比例大,核仁不明显。细胞核椭圆形、成团分布,上皮来源可能性大。
基于以上特点,我首先考虑良性:基底细胞腺瘤、多形性腺瘤(细胞丰富型)。
但是如果最后诊断是恶性,如腺样囊性癌(实性 solid type)、多形性低度腺癌,基底细胞腺癌,也在意料之中。因为这些恶性肿瘤的图像也可以这样。
想请教陈老师,这一例的报告该如何签发才合适?(比如:“涎腺来源肿瘤,低度恶性不除外,建议活检”)做细胞块(cell block)的免疫组化有帮助吗?
-
I think that people are in the right direction. I have said this many times here that if a salivary gland tumor lacks chondroid-myxoid stroma, I would not call this "pleomorphic adenoma" (PA) on cytology, even if by statistics, it might well be PA, thoes so called "cellular pleomorphic adenoma". I have the surgical resection of this tumor and it again teaches me that the category of the epithelial/myoepithelial tumor of the salivary gland includes a broad differential diagnosis. Anyone want to guess what the final pathology will be?











