
 - metastatic alveolar soft part sarcoma图1")
 - metastatic alveolar soft part sarcoma图2")
 - metastatic alveolar soft part sarcoma图3")
 - metastatic alveolar soft part sarcoma图4")
 - metastatic alveolar soft part sarcoma图5")
 - metastatic alveolar soft part sarcoma图6")
 - metastatic alveolar soft part sarcoma图7")
 - metastatic alveolar soft part sarcoma图8")


| 图片: | |
|---|---|
| 名称: | |
| 描述: | |
- NP (8) - metastatic alveolar soft part sarcoma
-
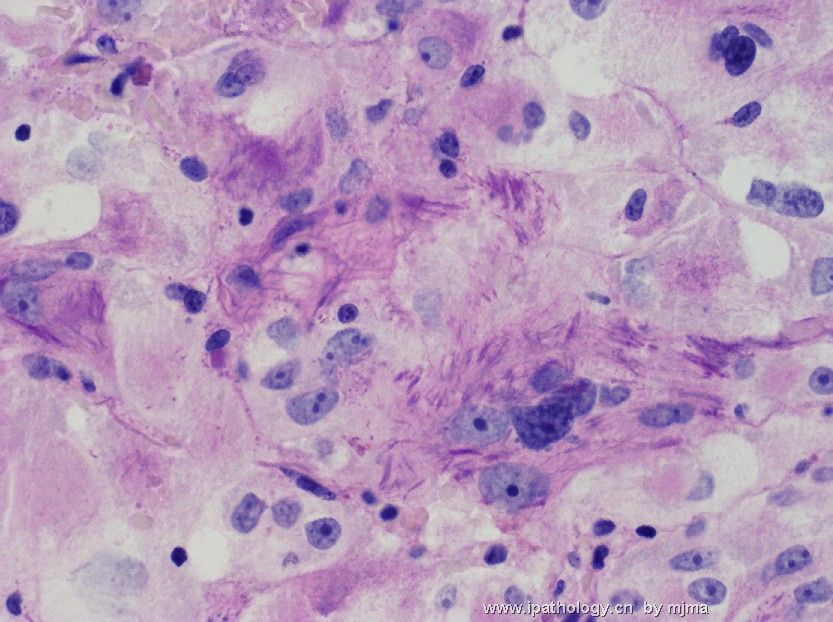
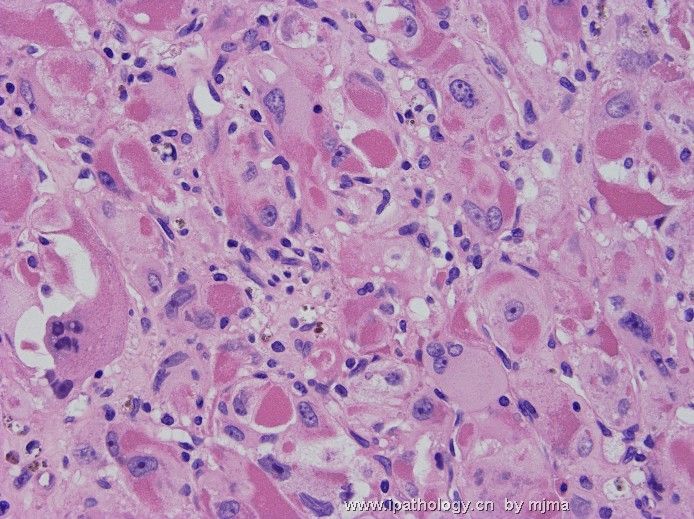
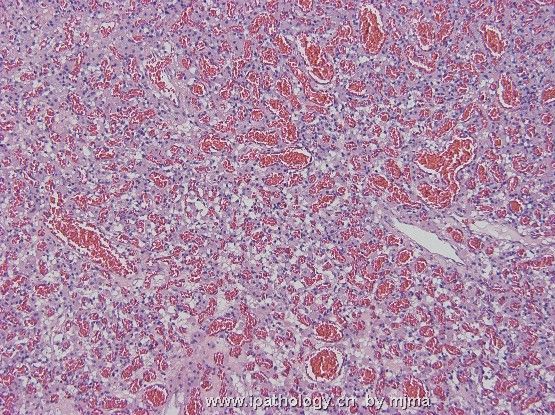
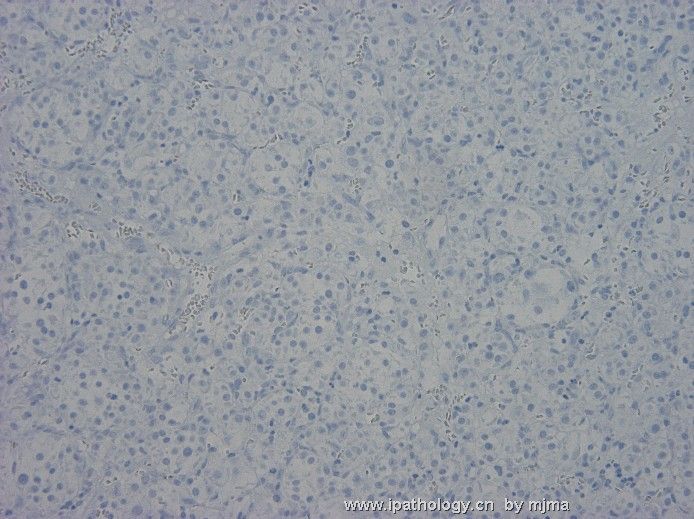
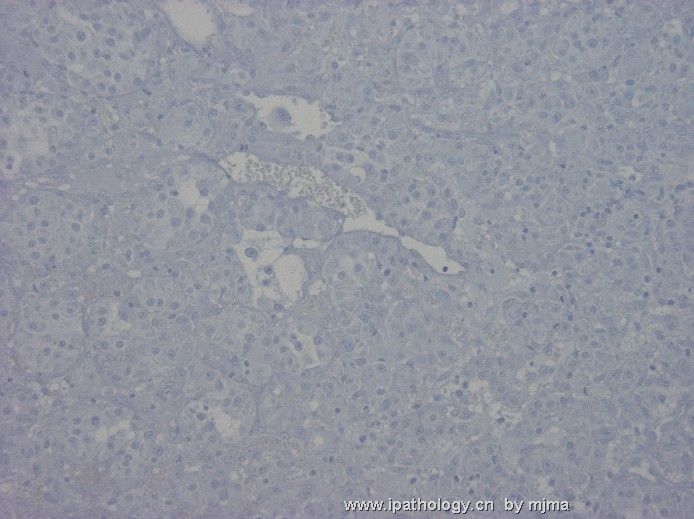
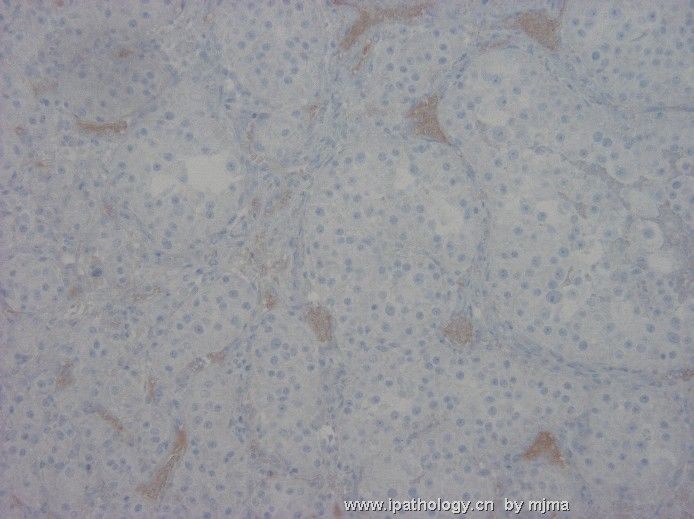
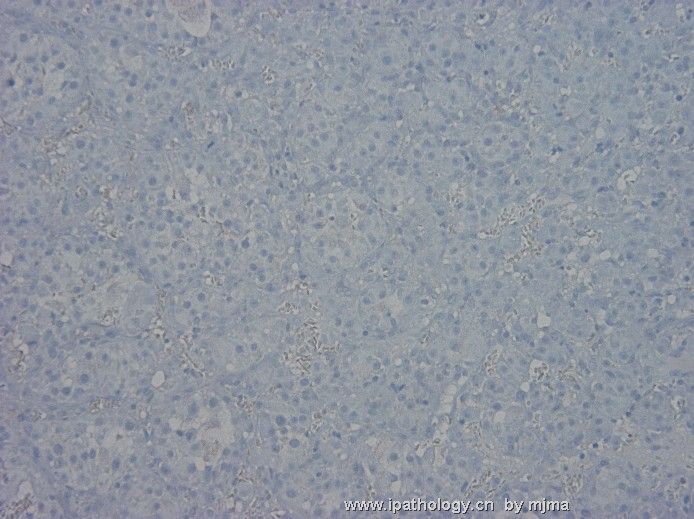
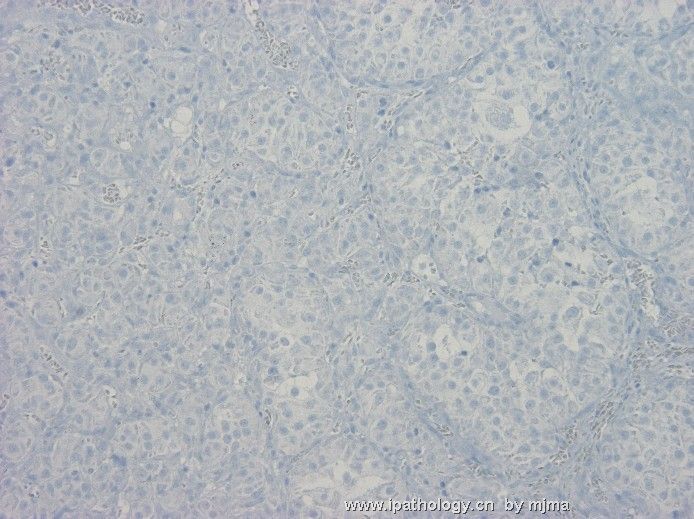
A 25-year-old man presented with new seizure disorder, and was found to have multiple enhancing lesions in the brain, spinal cord, none (vertebral column) and liver. The photos are taken from a resected left temporal lobe brain tumor. Figures 1~3 are from frozen section (HE) at magnification 10x, 20x and 40x. Figures 4~8 are from HE-stained paraffin section at magnification 4x, 10x, 20x, 40x and 60x. What are your differential diagnoses? What further workup do you suggest?
 - metastatic alveolar soft part sarcoma图1") 图1
图1 - metastatic alveolar soft part sarcoma图2") 图2
图2 - metastatic alveolar soft part sarcoma图3") 图3
图3 - metastatic alveolar soft part sarcoma图4") 图4
图4 - metastatic alveolar soft part sarcoma图5") 图5
图5 - metastatic alveolar soft part sarcoma图6") 图6
图6 - metastatic alveolar soft part sarcoma图7") 图7
图7 - metastatic alveolar soft part sarcoma图8") 图8
图8
标签:
-
本帖最后由 于 2008-02-17 22:31:00 编辑

聞道有先後,術業有專攻
×参考诊断
This is indeed a rare case of alveolar soft part sarcoma with wide spread metastases in liver, lung, bone and brain. It was extremely educational to me, and I wish to share what I learned with you.
The initial brain tumor removed from this young man generated a long list of differential diagnoses of metastatic nature (no primary brain tumor has such histopathology). Those I considered seriously are (1) renal cell carcinoma (chromophobe variant of high nuclear grade), (2) hepatocellular carcinoma and hepatoblastoma, (3) Leydig cell tumor of testicular origin, (4) paraganglioma or pheochromocytoma, (5) oncocytic carcinoma of thyroid gland, salivary gland, or pancreatic origin, and (6) melanoma. Extensive immunohistochemical staining showed mild to moderate immunoreactivity to synaptophysin and strong immunoreactivity to neuron-specific enolase (NSE). Except for paraganglioma/pheochromocytoma, all of my other differential diagnoses were ruled out. After I exhausted my wisdon, I sent the case to a friend of mine, who told me the correct diagnosis after looking at the slides for 10 minutes. I stained it for PAS with diastase pretreatment, and saw NO CYTOPLASMIC PAS-POSITIVE CRYSTALS (the photos of PAS-positive crystals shown above were taken from the vertebral tumor resected later). Diagnostic electron microscopy and TFE3 immunostain were subsequently done and the diagnosis was confirmed.
Alveolar soft part sarcoma is rare. It often occurs in the extremities of young males. It is a highly aggressive malignancy of unclear histogenesis. Patients often present with symptoms related to metastastatic disease (seizure or weakness from CNS mets and pain from bone mets are most common) while the primary tumor remains either undetected or appears indolent (as is this case) at the time of presentation. Advanced stage (widespread metastases above and below diaphragm). After the suspicion of metastatic alveolar soft part sarcoma was raised based on the removed brain tumor, the patient was questioned and he reported a "leg mas" that had been present for a few months. Physical examination revealed a deeply seated, large soft tissue mass in his left upper calf. MRI showed this heterogeneously enhancing mass to be about 8 x 6 x 6 cm in size, and was in the muscles and fascia. Fine needle aspiration revealed neoplastic cells similar to those found in the brain (and subsequently, in the vertebral tumor).
It would not be necessary for me to copy what textbooks write about this fascinating malignancy here. I would encourage you read about the disease in updated textbooks or recent journals. A good summary by Weiss appeared 5 years ago in the American Journal of Pathology. It is available online at http://ajp.amjpathol.org/cgi/content/full/160/4/1197. A more recent review article by Folpe and Deyrup in 2006 is also available online at http://jcp.bmj.com/cgi/content/full/59/11/1127.
To summarize my lessons learned from this case: (1) never undervalue a complete history taking and physical examination, (2) PAS can be negative for alveolar soft part sarcoma, and (3) recognize my limitations and respect/welcome a second opinion from a colleague. I hope I will never miss this diagnosis again.
聞道有先後,術業有專攻
-
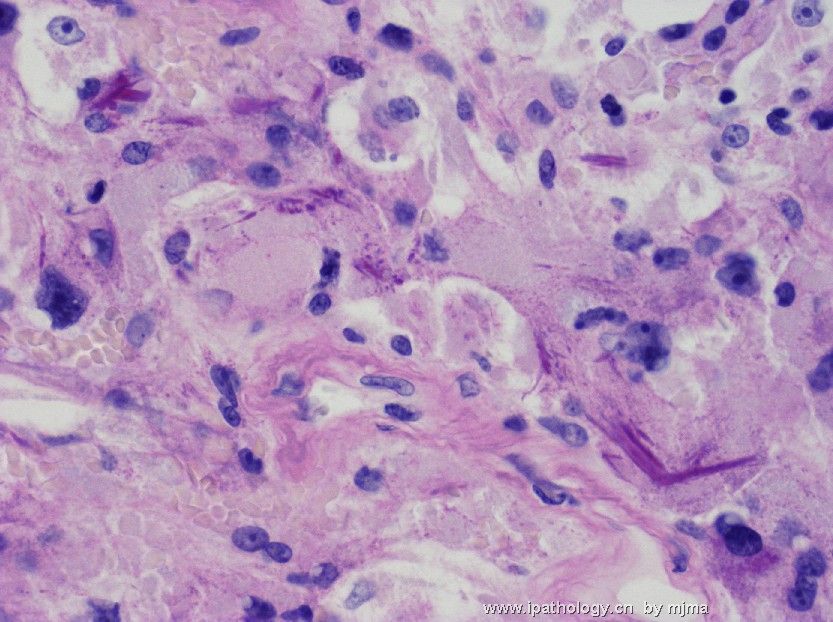
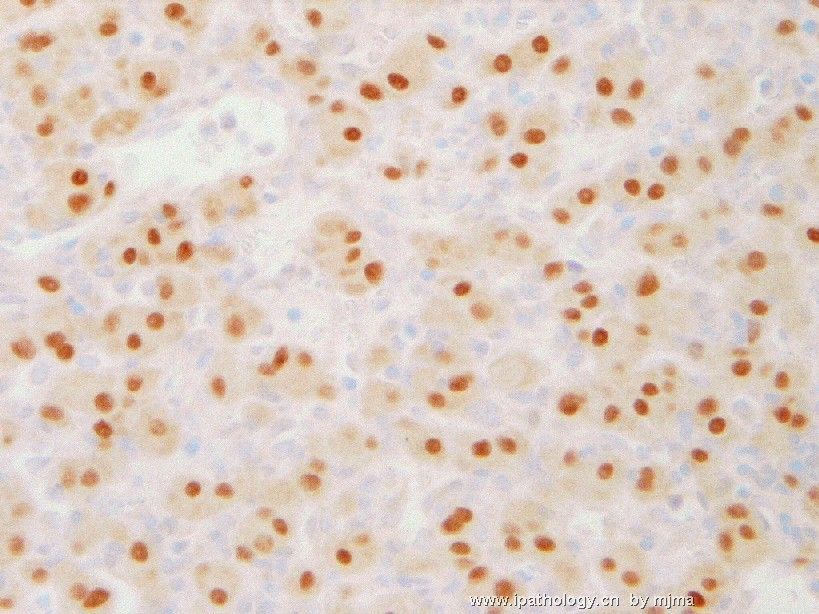
Figures 1~2 are from PAS stain after diastase pretreatment, figures 3~4 are electron micrographs taken from neoplastic cells, and figure 5 is an immunohistochemical stain of neoplastic cells using an antibody against TFE3 (transcription factor 3). These additional information led to the definitive diagnosis, which will be announced shortly. What do you think this is?
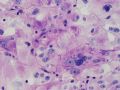 图1
图1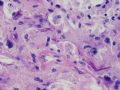 图2
图2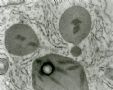 图3
图3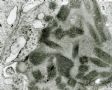 图4
图4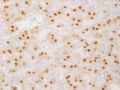 图5
图5
聞道有先後,術業有專攻
-
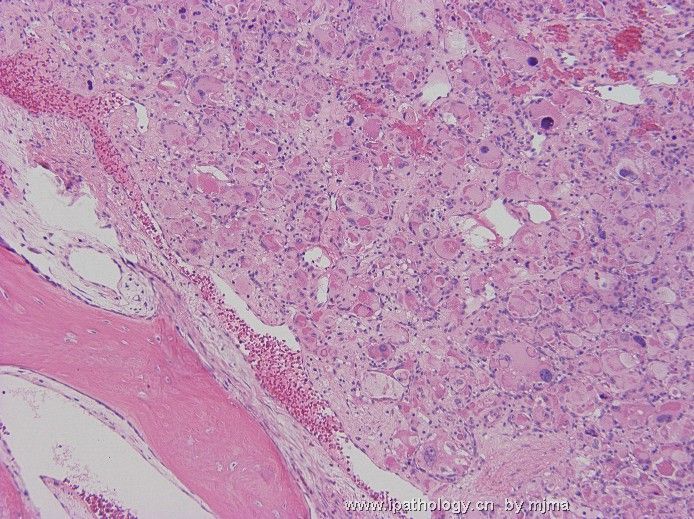
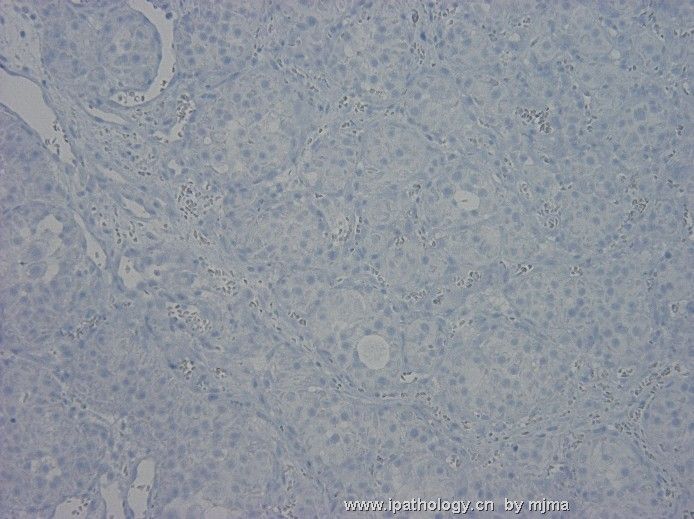
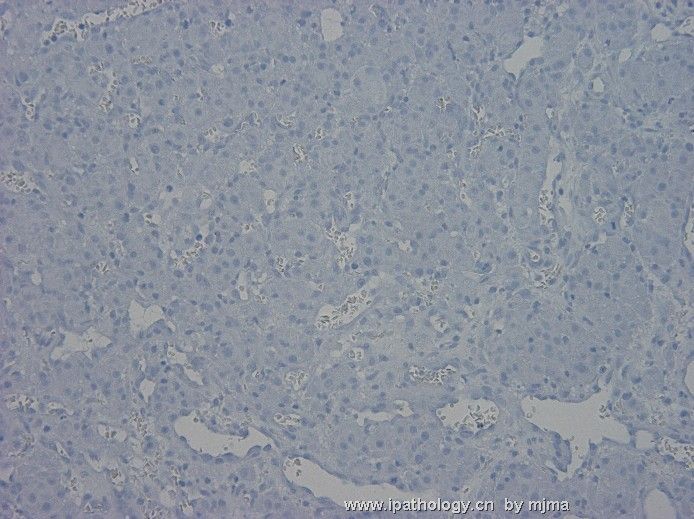
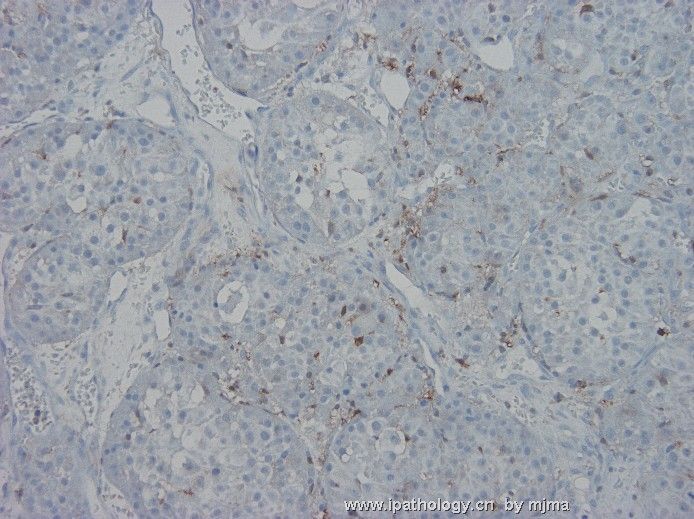
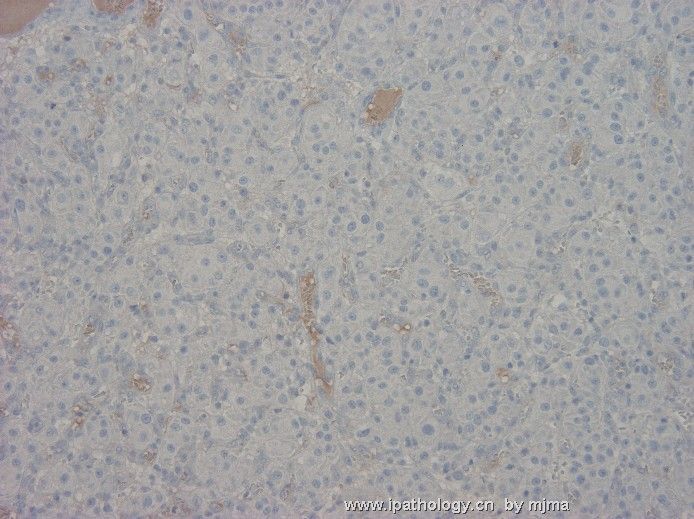
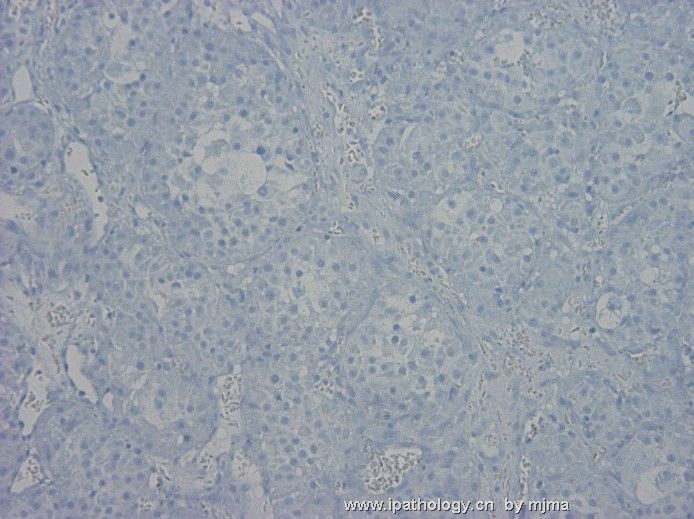
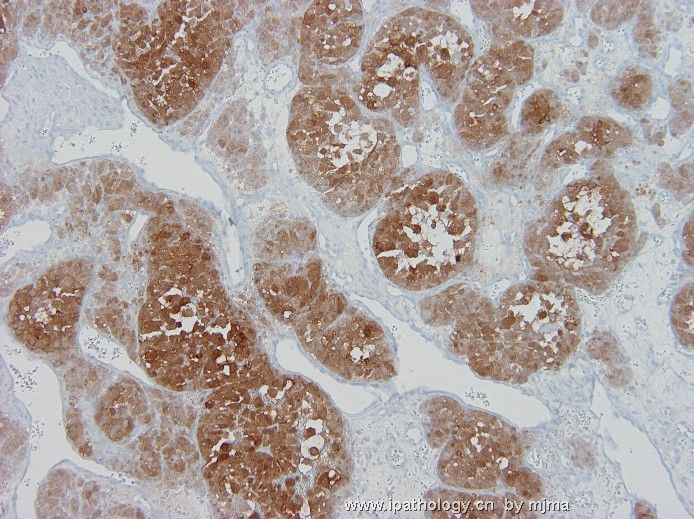
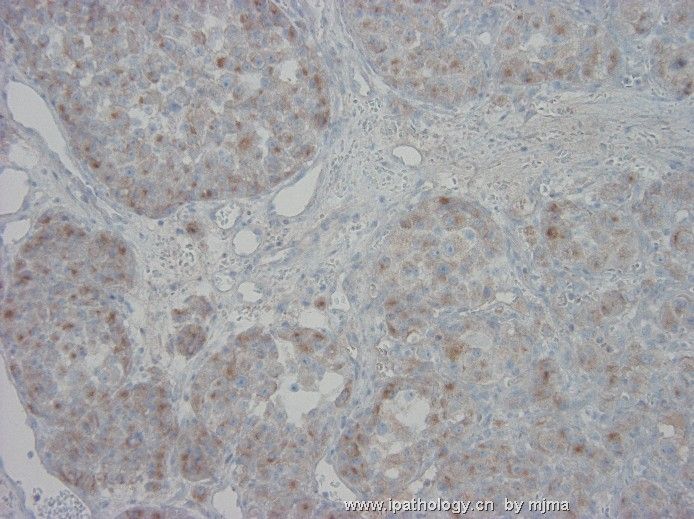
A few days later, a vertebral bone destructive lesion compressing the spinal cord was removed during decompression surgery, and photos 1~3 below were taken from the lesion. Multiple immunohistochemical stains were done, some of which were presented here: Figure 4 - AE1, 5 - Cam5.2, 6 - EMA, 7 - HepPar-1, 8 - alpha-fetoprotein, 9 - S100 protein, 10 - Melan-A, 11 - chromogranin A, 12 - neuron-specific enolase (NSE), 13 - synaptophysin, 14 - GFAP, and 15 - inhibin. What do you think?
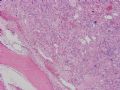 图1
图1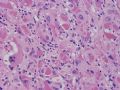 图2
图2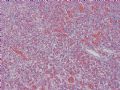 图3
图3 图4
图4 图5
图5 图6
图6 图7
图7 图8
图8 图9
图9 图10
图10 图11
图11 图12
图12 图13
图13 图14
图14 图15
图15
聞道有先後,術業有專攻











