
图1")
图2")
图3")
图4")
图5")
图6")
图7")
图8")
图9")
图10")






| 图片: | |
|---|---|
| 名称: | |
| 描述: | |
- 2009-7-21前臂肿瘤(再传图)
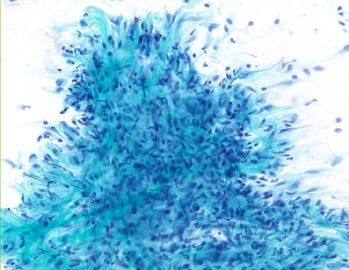 图1
图1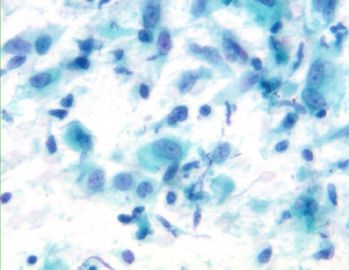 图2
图2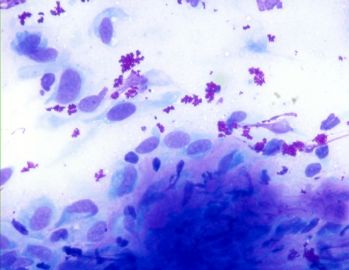 图3
图3
Hi LjmLjm: I saw your post briefly yesterday and was not all clear. But I get the sense that this case might be a sarcoma of some kind. I just want to clarify that before you diagnose sarcoma on FNA, you need to exclude benign lesions of the soft tissue, such as nodular fasciitis, cellular schwannoma, and etc, which can mimic sarcoma.
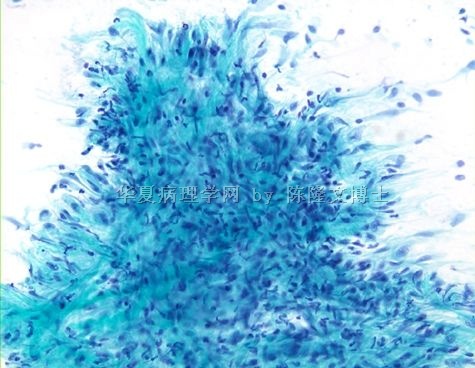
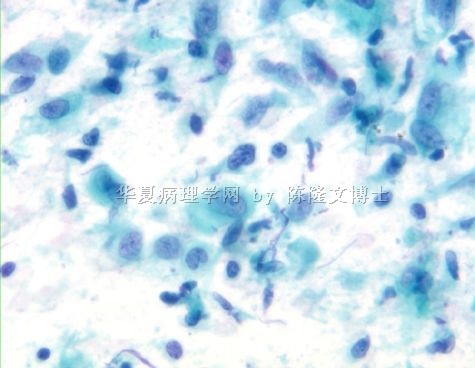
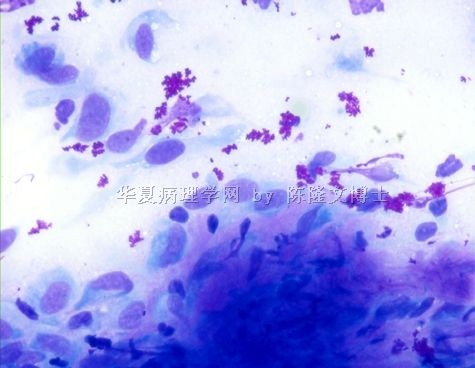
Let me post a FNA example of very cellular nodular fasciitis. The case was shown at the USCAP meeting evening cytopathology interesting case conference, more than half of the expert cytopathologists called it sarcoma.
This is a very interesting case and also brings a discussion of soft tissue FNA. FNA for primary diagnosis of soft tissue tumors can be very challenging and difficult. In my Department, we have 3 famous soft tissue pathologists including my chairman (JRG), who is the principal author of the world most popular soft tissue text book. Sometimes, on some small excisional biopsies, he cannot be definitive on the diagnosis, so FNA has limited use. But, if a patient already has a soft tissue tumor diagnosis established, FNA can be used to check recurrence or metastasis.
Back to the case, I completely 菊形团's comment. 结节性筋膜炎 need to be considered. Reactive myofibroblasts/fibroblasts usually have this "tissue culture cells" appereance (the last 2 photos), they can be very cellular but not hyperchromatic. Mistaken 结节性筋膜炎 for soft tissue sarcoma is the most common one in soft tissue pathology and it can be avoided if you think about 结节性筋膜炎. If you are not sure, you can call this case "atypical spindle cells proliferation" and recommend surgical excision for final diagnosis.











