







| 图片: | |
|---|---|
| 名称: | |
| 描述: | |
- A challenging head and neck FNA
-
本帖最后由 于 2009-07-01 01:02:00 编辑
译陈博士: I feel that this case is very difficult and I would like to summarize it:我觉得诊断本例非常困难,现小结如下:
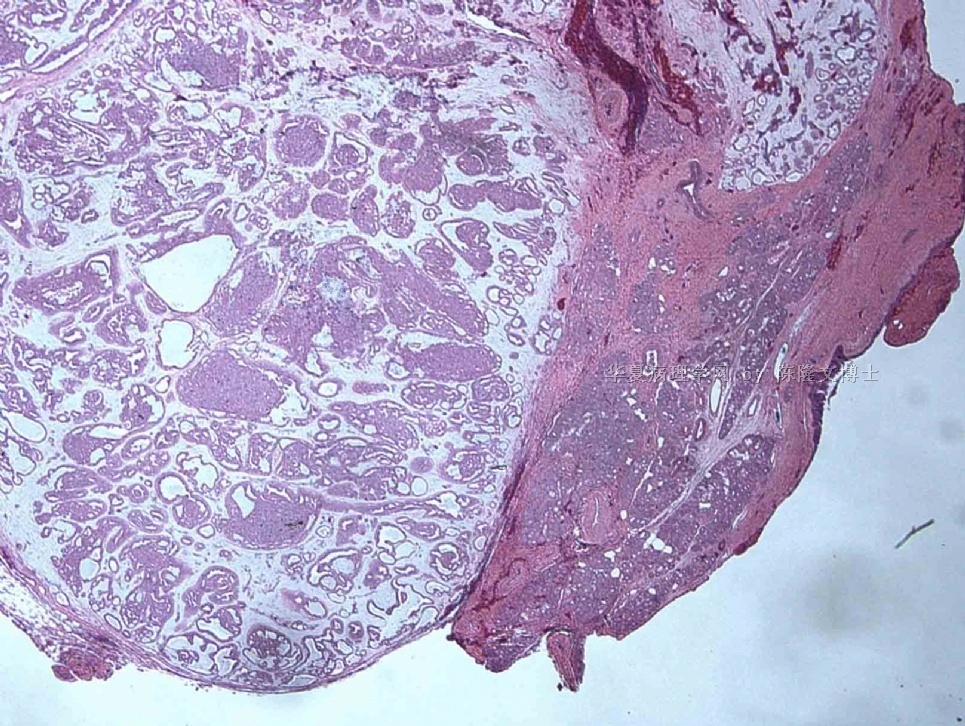
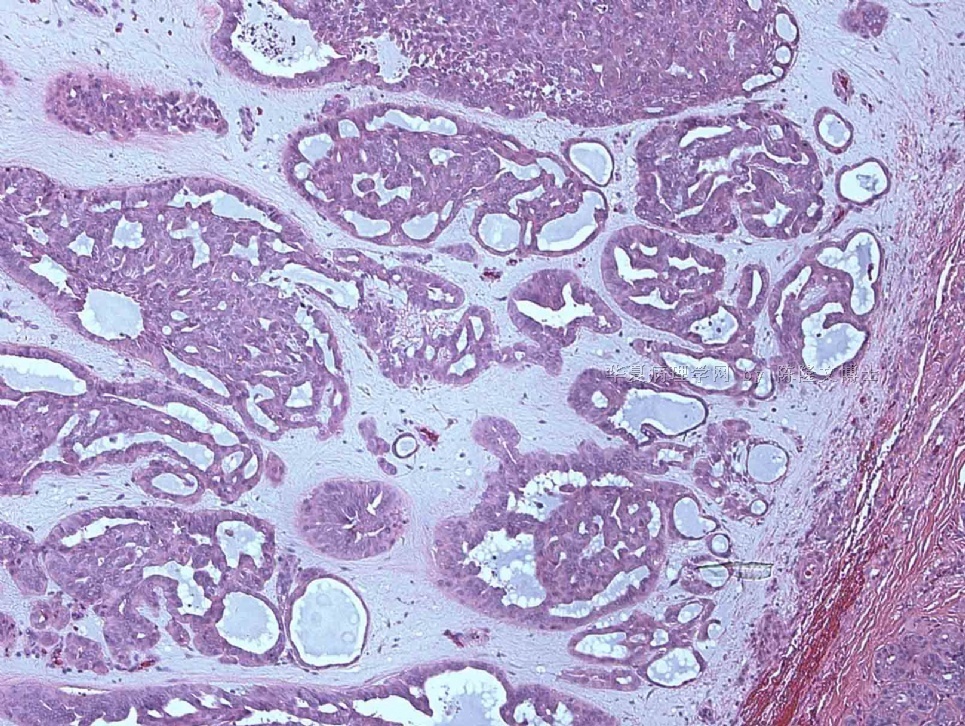
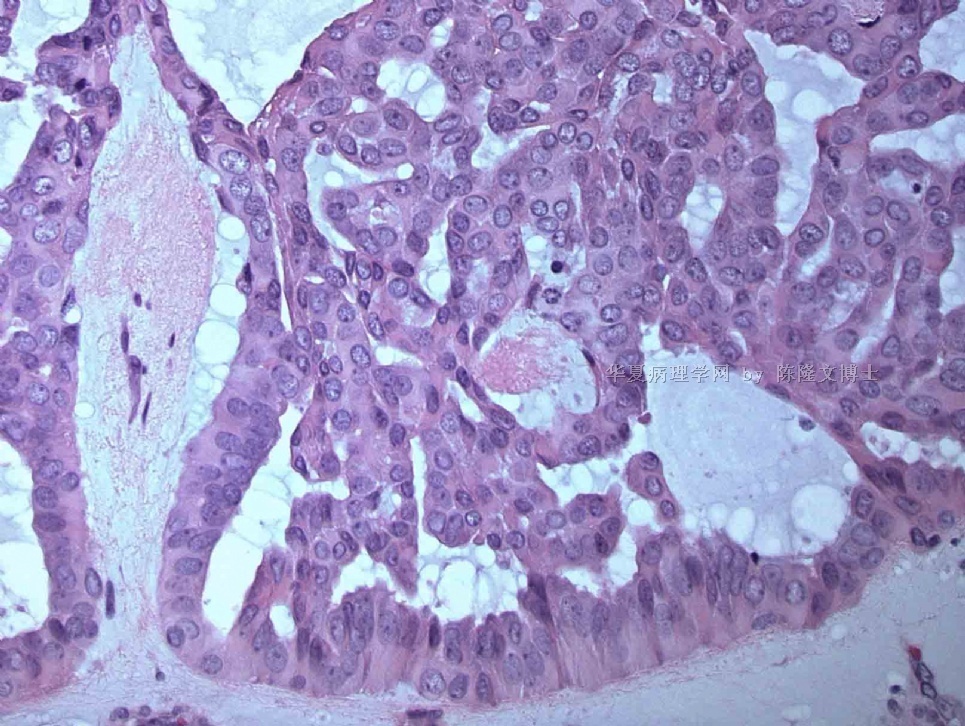
1) Polymorphous low-grade adenocarcinoma (PLGA) is found almost exclusively in minor salivary gland. 1)多形性低级别腺癌 (PLGA)几乎都发生在小涎腺,It is a low-grade malignancy with generally good prognosis. 其为低度恶性的肿瘤,通常愈后较好,It is commonly present in patients aged 50-70 year-old with female affected twice as frequently as men (our patient is a 61-year-old woman).多见于50-70岁之间,女性比男性多发,约高于男性两倍的发病率.本例也为一61岁的女性患者.2) PLGA is cytologically uniform, but architecturally diverse:2)PLGA细胞虽然比较一致,但是结构有差别,it can be lobular, solid nests, cribriform, or papillary.可以呈小叶状,实体,巢状,筛状或呈乳头状结构. It is usually infiltrative with perineural invasion. 瘤细胞常浸润到神经周围,The bluish stroma in the background is typical and it is different from the chondroid myxoid stroma found in pleomorphic adenoma (PA);本例细胞团块的蓝色背景是非常典型的,它不同于多形性腺瘤的软骨粘液样背景,3) The differential diagnosis of PLGA mainly includes PA and adenoid cystic carcinoma (ACC). 3)本例需要与多形性腺瘤,腺样囊性癌区别.Because PLGA has diverse architectural appearance, it is very difficult to diagnose on FNA and most of times are not possible even on small excisional biopsy. 由于这种多形性低级别腺癌在细针穿刺细胞涂片时难以诊断,甚至经常在小块组织活检时也难以做出诊断,This patient had a small excisional biopsy almost 10 years ago and was called PA, but we get the outside slides and it is almost identical to the current resection specimen, also showed perineural invasion.患者在十年前小块切除活检就被误诊为多形性腺瘤,我们借到他十年前活检切片,和这次手术切除标本几乎完全一样,在切片中均显示肿瘤浸润到了神经周围,4) This case brought a very important concept that I would like to share with our chinese pathologists on ipathology. 4)本例给我们提出一个非常重要的概念,我提出并与咱们华夏病理网友们分享.Salivary gland FNA can be very difficult, 涎腺的FNA诊断是非常困难的,if a FNA sample does not fit perfectly in a disease category, 如果不能精确分类时,,I would have no hesitation to issue the report with "Atypical cells present" and a comment recommend excision. 我们不要犹豫,可以直接签发报告为查见有非典型性细胞,建议手术切除.In this case, on the FNA, I don't see the typical chondroid-myxoid stroma, so I would not just sign out the case as "pleomorphic adenoma"本例,.我没有看到典型的软骨粘液基质,我没有发可能是多形性腺瘤的报告,5) To be a good cytopathologist, 5)做为一个好的细胞病理学家,we have to know our limitation and the clinical management, 我们必需知道我们的诊断的界线,也更要知道临床的处理方法,as most of the salivary gland tumors will be clinically taken out surgically anyway except some Warthin tumors, metastatic tumors, and lymphoma. 要明白,多数的涎腺肿瘤都要做及时手术,完整切除,除了某些乳头状淋巴囊腺瘤,转移癌和淋巴瘤,这些肿瘤可能不必要及时手术.So, if you can tell the clinician that this is most likely a low-grade salivary gland neoplasm (not Warthin tumor or lymphoma or metastatic tumor),因此,如果你告诉临床医生,这个肿瘤是低级别涎腺肿瘤,不是乳头状淋巴囊腺瘤,转移癌和淋巴瘤, the clinical management usually is similar.临床处理是一样的.
I feel that this case is very difficult and I would like to summarize it:
1) Polymorphous low-grade adenocarcinoma (PLGA) is found almost exclusively in minor salivary gland. It is a low-grade malignancy with generally good prognosis. It is commonly present in patients aged 50-70 year-old with female affected twice as frequently as men (our patient is a 61-year-old woman).
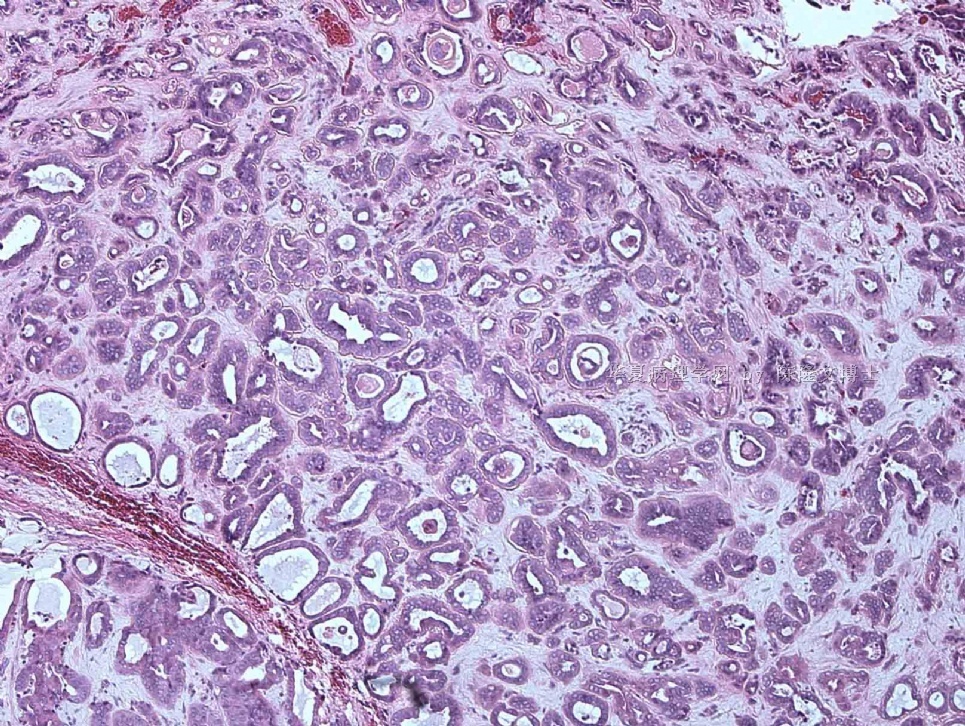
2) PLGA is cytologically uniform, but architecturally diverse: it can be lobular, solid nests, cribriform, or papillary. It is usually infiltrative with perineural invasion. The bluish stroma in the background is typical and it is different from the chondroid myxoid stroma found in pleomorphic adenoma (PA);
3) The differential diagnosis of PLGA mainly includes PA and adenoid cystic carcinoma (ACC). Because PLGA has diverse architectural appearance, it is very difficult to diagnose on FNA and most of times are not possible even on small excisional biopsy. This patient had a small excisional biopsy almost 10 years ago and was called PA, but we get the outside slides and it is almost identical to the current resection specimen, also showed perineural invasion.
4) This case brought a very important concept that I would like to share with our chinese pathologists on ipathology. Salivary gland FNA can be very difficult, if a FNA sample does not fit perfectly in a disease category, I would have no hesitation to issue the report with "Atypical cells present" and a comment recommend excision. In this case, on the FNA, I don't see the typical chondroid-myxoid stroma, so I would not just sign out the case as "pleomorphic adenoma".
5) To be a good cytopathologist, we have to know our limitation and the clinical management, as most of the salivary gland tumors will be clinically taken out surgically anyway except some Warthin tumors, metastatic tumors, and lymphoma. So, if you can tell the clinician that this is most likely a low-grade salivary gland neoplasm (not Warthin tumor or lymphoma or metastatic tumor), the clinical management usually is similar.
-
译文: I do NOT see the typical fibrilary chondroid-myxoid stroma in this case, so I could not call this case pleomorphic adenoma.我没有看到本例有典型的纤维软骨样粘液基质, I decided to sign out as " a low grade epithelial neoplasm", recommend excision.我签发的病理报告:低级别上皮性肿瘤,建议手术切除。 It turned out to be a very good case of ????, 结果是一例非常有趣的病例,Can you guess?大家能猜出来吗?
I have the surgical resection of this tumor and will post soon.我有组织学切片,不久会帖出来供大家欣赏。
I do NOT see the typical fibrilary chondroid-myxoid stroma in this case, so I could not call this case pleomorphic adenoma. I decided to sign out as " a low grade epithelial neoplasm", recommend excision. It turned out to be a very good case of ????, Can you guess?
I have the surgical resection of this tumor and will post soon.











