

| 图片: | |
|---|---|
| 名称: | |
| 描述: | |
- B1752Breast lesion DCIS or ADH cqz (8)
Today I had two cases and send here to see what you think. I feel interesting.
今天上传两例,看看大家考虑什么。我觉得很有意思。
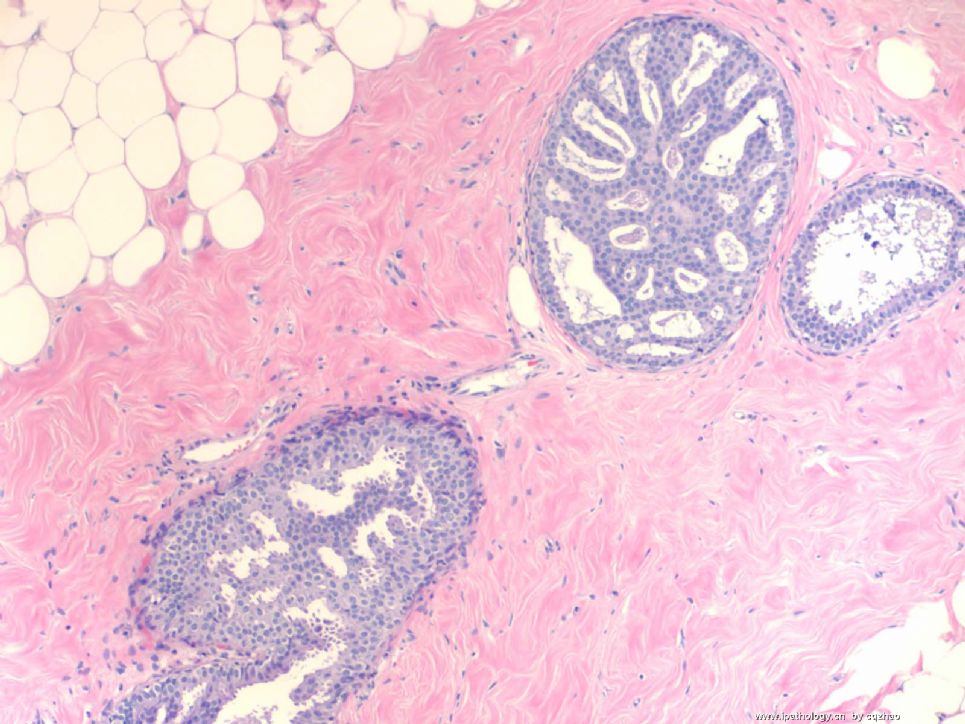
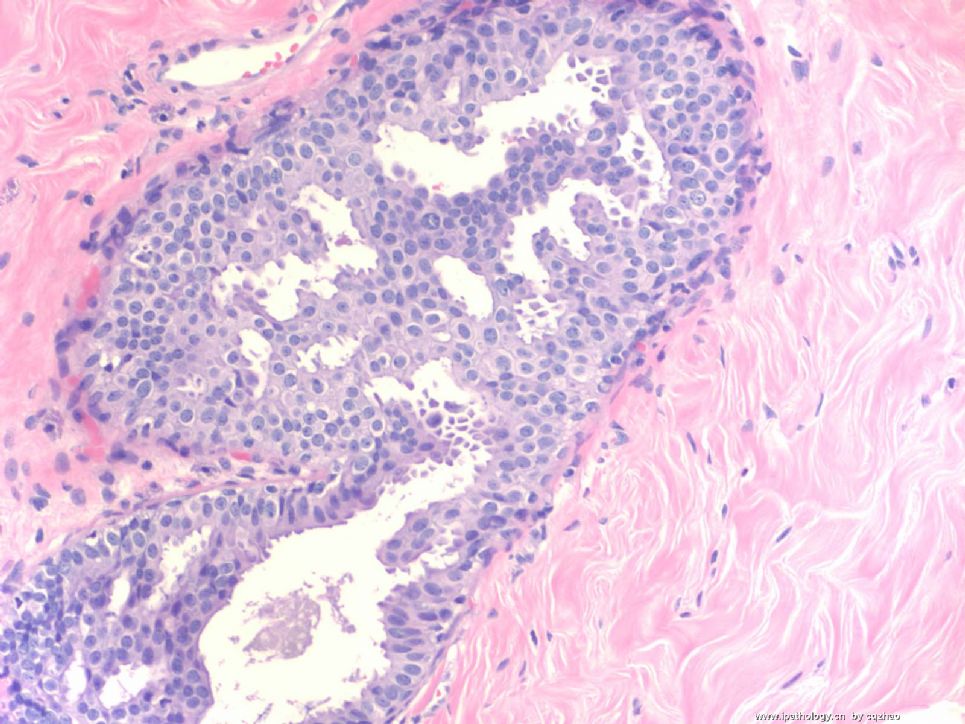
Case 1. About 80 y. Previous core bx was reported as focal ADH. Today I had segmental mastectomy. Only focal atypical proliferation (fig 1 100x, fig 2-3 200x) was noted. The focal area measures 2 mm (2 ducts), closely to the previous biopsy area.
病例1 约80岁。以前粗针活检报告为局灶性ADH。今天的区段切除标本,注意到也仅有局灶性不典型增生(图1 100倍,图2-3 200倍)。局灶区域大小2mm(2个导管),与以前活检区域很靠近。
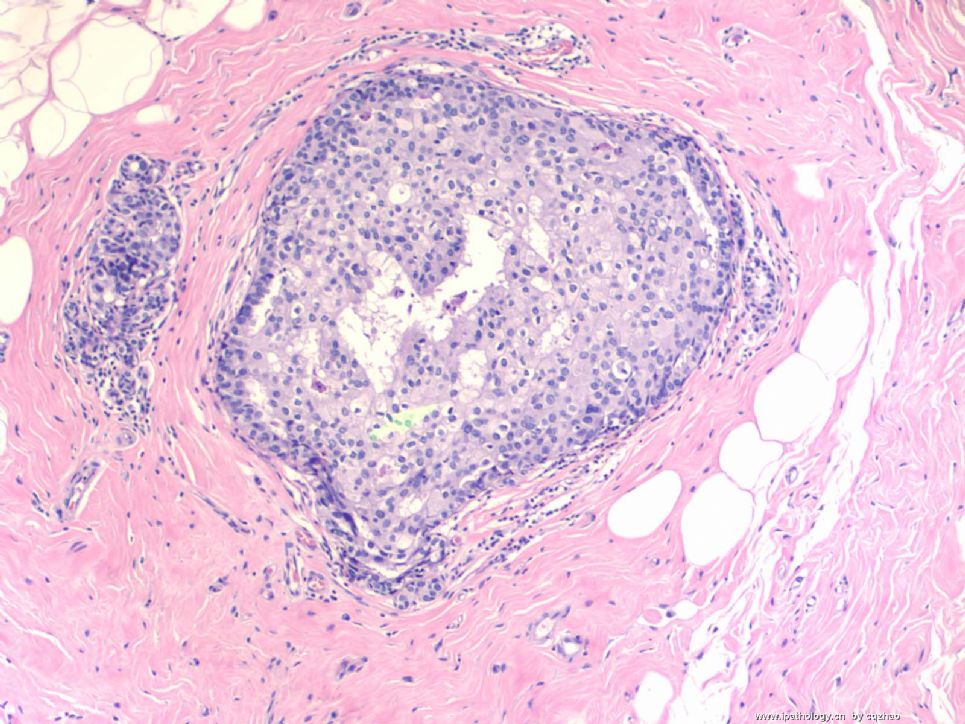
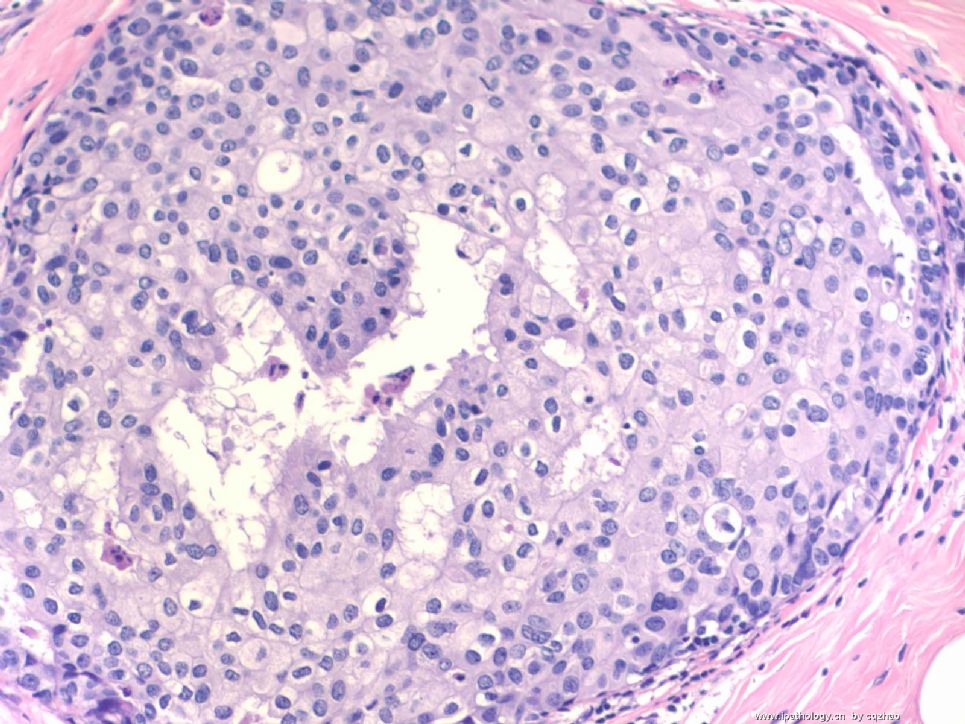
Case 2. about 50 y. Previous core biopsy was reported as DCIS, nuclear grade 2. Atypical proliferation was noted in one duct as fig (fig 4 100x, fig 5 200x), closely to the previous biopsy area.
病例2 约50岁。以前粗针活检报告为DCIS,核级别2级。注意到一个导管内的不典型增生,如图(图4 100倍,图5 200倍),与以前活检部位接近。
All specimens were submitted for microscopically examination, one with 45 slides and other with 57 slides.
所有标本均切片,分别为45张和57张切片。
Pleae choose:
A. Both ADH
B. Both DCIS
C. Case 1 ADH, case 2 DCIS
D. Case 1 DCIS, case 2 ADH
请选择:
A。均为ADH
B。均为DCIS
C。病例1为ADH,病例2为DCIS
D。病例1为DCIS,病例2为ADH
Please choose one from A, B, C, D. Hope all people who see the photos can write your choice. Will appreciate if you can write why. Do not worry it is no right or wrong answer. Just interested to see how pathologists interpretate these kinds of lesions.
请从ABCD中选择一项。希望所有看过图片的人都写下选择。如果写上为什么(诊断依据)更好。不要担心对或错。仅仅想看看病理医生们是如何解释这种病变的。
You need to review breast books if you want to call them as UDH.
如果你想称之为UDH,那你需要复习一下乳腺病理的专著。
标签:ADH DCIS
-
本帖最后由 于 2008-12-14 19:41:00 编辑
相关帖子
- • 乳腺包块
- • 左乳癌标本乳头一个导管内的病变
- • 乳腺两个相邻导管内的病变
- • 乳腺肿物
- • 乳腺肿物,请各位老师帮忙会诊
- • 女 46岁发现左乳腺肿块一月余
- • 乳腺包块。33岁
- • 左乳肿块,协助诊断
- • 乳腺肿物
- • 乳腺肿物
×参考诊断
I almost forget this case. Thank 天山望月 for mentioning this case. The original purpose i showed this case here was to demonstrate that some cases in pathology are bordeline cases. Different pathologists in different hospitals can have variable interpretation. Breast proliferative lesions can be continuous, UDH-ADH-DCIS. I once mentioned this somewhere in the website even though some pathologists did not agree with me. We need to consider the natures of the lesions and all other condition when we make a diagnosis. The importance is that what clinicians will do when they read our reports. For above cases I reviewed previous breast core biopsy specimens to confirm the diagnosis.
For case one: 80 y lady with ADH in core biopsy. Current segmental specimen only showed focal atypical proliferation involving two ducts with monotanous cell population and cribriform growth pattern. I sign out focal ADH. I do not want to give a new diagnosis of cancer for this 80 years older lady, as abin mentioned above.
For case 2: 50 y lady with DCIS in previous core biopsy. Current segmental specimen only showed atypical proliferation involving one dcut with solid pattern which was close to prvious biopsy site. Cytomorphologic features are exactly the same as that in previous biopsy specimen. I feel confident it was part of lesion of DCIS in core biopsy. I called this case focal DCIS. I am ok if some one called ADH for the focal lesion. It is far from the margin. Whatever you call will not change the following treatment of the patient. The very difficult situation is that if the focal lesion is close to or in the margin. if we call DCIS in the margin, the surgeons may do another segmental mastectomy. If we call ADH (currently we do not report margin for ADH), the women will have no other surgery. Pathologists' diagnoses may direct the treatment of the patients. It indicates not only the importance of our work, but also the responsibility and the risk of work.
Case 1: dx of ADH may be better.
Case 2: either adh or dcis.
Bottom line you should call UDH.
I reviewed the topic of 转录乳腺纠纷鉴定报告,病理医生可以从中学到些什么"
It is great that most pathologists mentioned "careful, careful, and more careful" "asking" when we release the cases. Of cause no person is perfect even older experts.
Ok, now I can close this case. Thank people join in the discussion. I think this case is very easy to answer, just typing a, b, c, d. However there are still few people made your choice. Interesting...











