




| 图片: | |
|---|---|
| 名称: | |
| 描述: | |
- FNA of lung mass
-
This is a 41-year-old female with one left upper lobe lung mass in June 2008 and now has one new left lower lobe lung mass. The FNA was done in June 2008 in an outside hospital. They used the rapid H&E stain (our pathologist friends in China are more familia with this stain). The patient has a history of a lower leg mass back in 2001 (I don't know the diagnosis and is in the process of getting the slides). The outside pathologist made a diagnosis on the FNA, which is reasonable but I doubt it. The first three pictures are cytology and the last two pictures are the cell block. Should generate some discussion? I will keep you posted.
 图1
图1 图2
图2 图3
图3 图4
图4
标签:
×参考诊断
转移性滑膜肉瘤
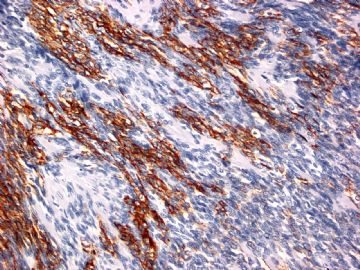 图1
图1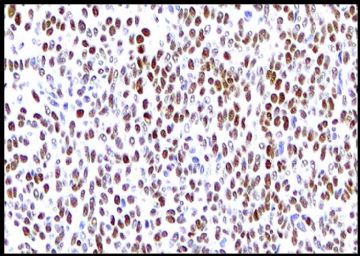 图2
图2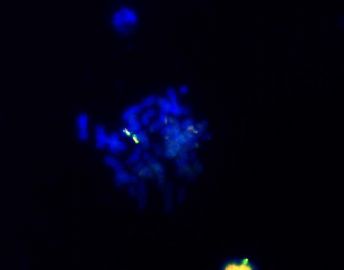 图3
图3
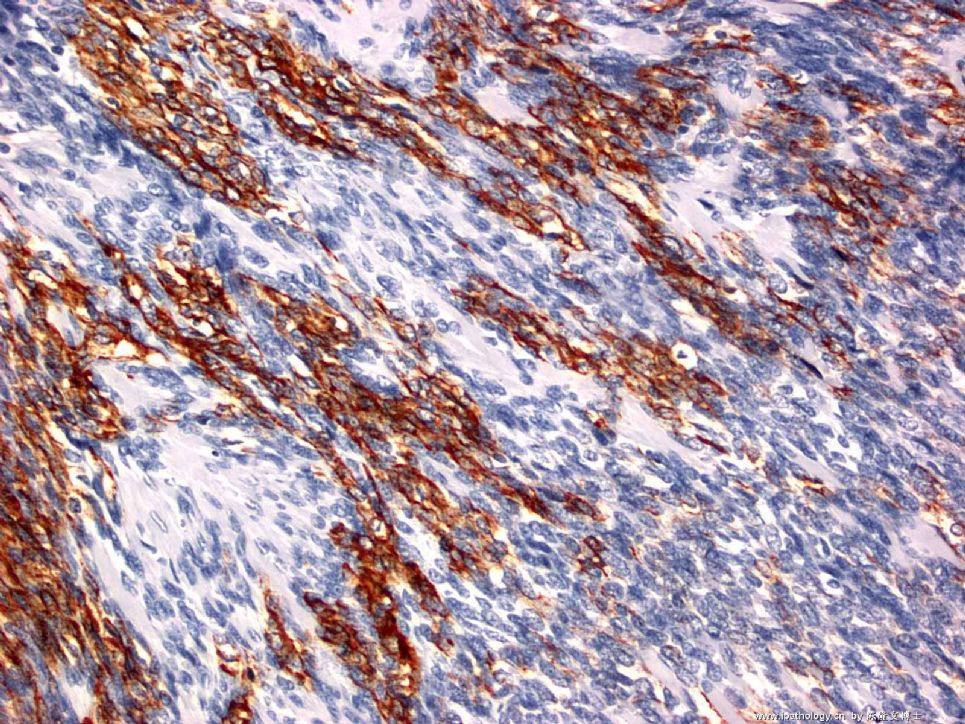
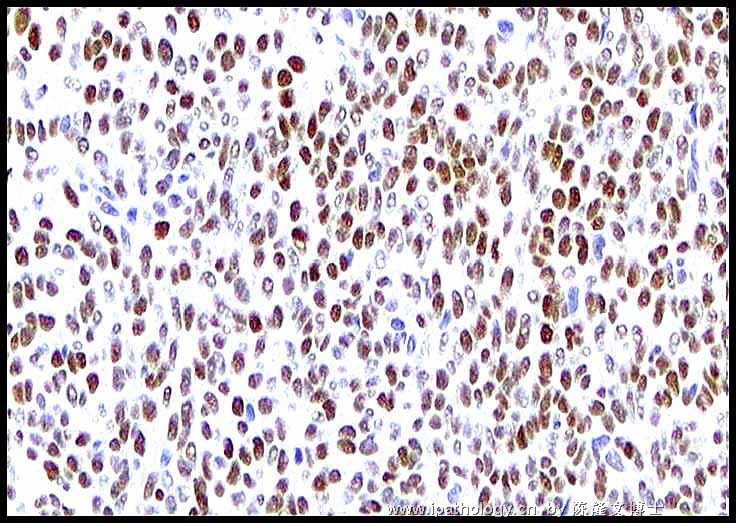
I think that this is a metastatic synovial sarcoma. Because of the wrong diagnosis, the patient's lung nodule got resected and did NOT go for the appropriate chemotherapy. But, we need to respect other pathologist's opinion. It will be not responsible to just sign this case out without doing any further studies. So, I did two more immunostaines on the block:
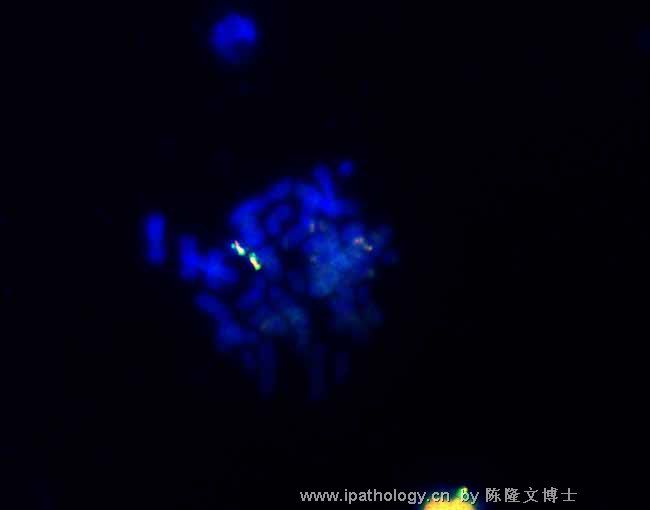
1) CK19, which should be positive for synovial sarcoma; 2) TLE-1: we use that a lot for our soft tissue service to diagnose synvial sarcoma (Terry et al. TLE1 as a diagnostic marker for synovial sarcoma emerging from gene profile study. American Journal of Surgical pathology, 31:240-6, 2007): this stain should be nuclear staining. I also did FISH study on the cell block and it is POSITIVE for SYT gene.
Final diagnosis: metastatic synovial sarcoma.
Note: synovial sarcoma can be focally positive for Synaptophysin, when you do immunostains, be careful to interprete immunostains, your diagnosis should not be solely depend on 1 or 2 positive immunostains, it has to be correlate with morphology and clinical presentation.
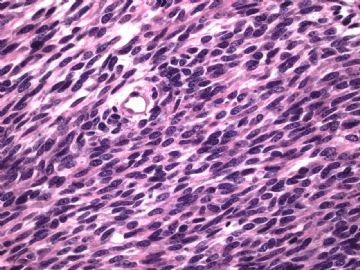 图1
图1
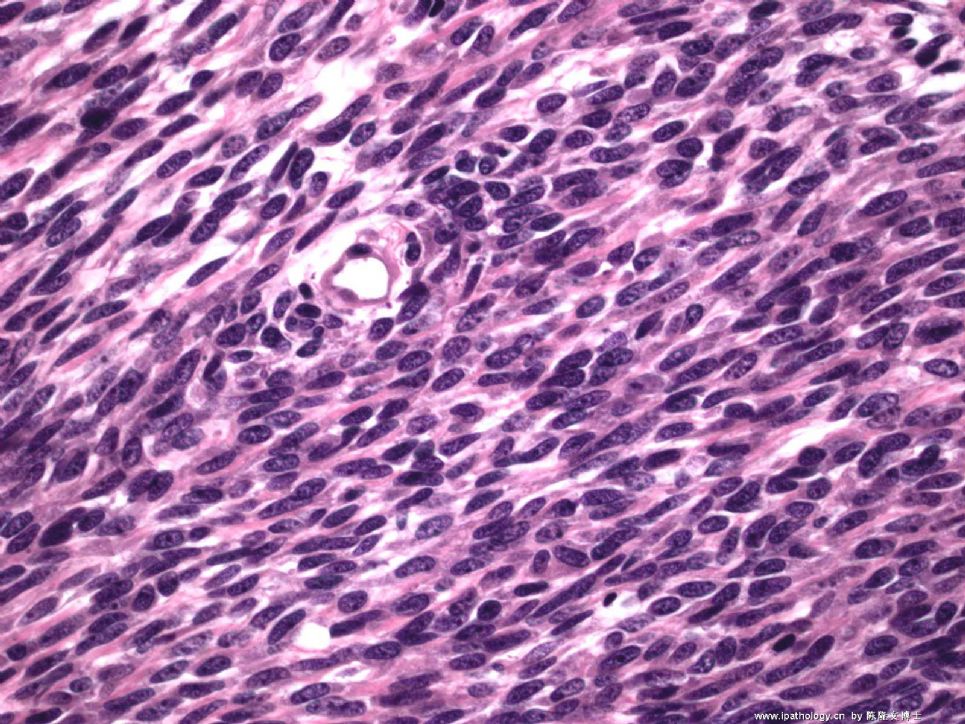
OK. I got the outside slides (2001) from this patient's previous soft tissue mass, it is synovial sarcoma. The pictures are shown here. The outside pathologist called this lung mass "neuroendocrine carcinoma, favor atypical carcinoid tumor". They did immunohistochemistry on the current lung nodule (I did not get the IHX slides), it is positive for cytokeratin AE1/AE3 and synaptophisin. the tumor cells are negative for Chromogranin.
Is this metastatic synovial sarcoma or a second primary lung neuroendocrine tumor? What extra-immuno or test you would do to support your diagnosis? or you are so confident that you just want to sign out this case. I ordered some extra tests and will keep you posted tomorrow.











