
























| 图片: | |
|---|---|
| 名称: | |
| 描述: | |
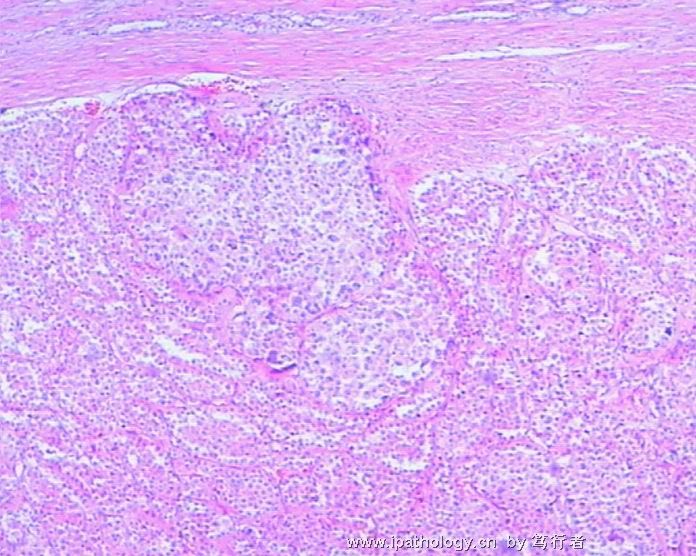
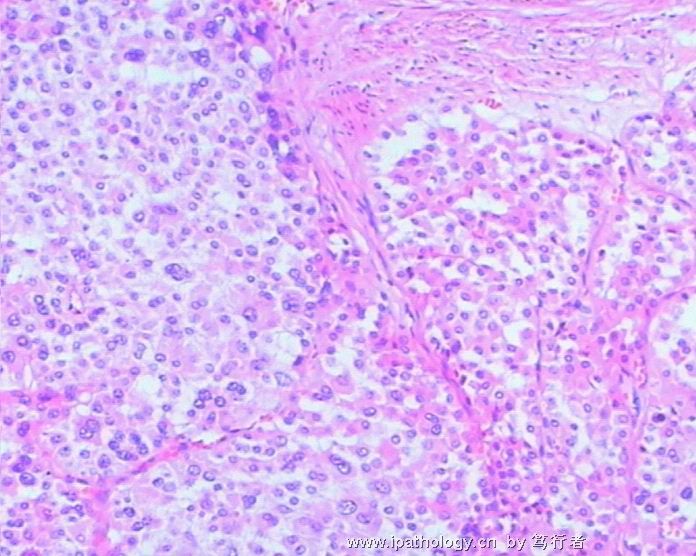
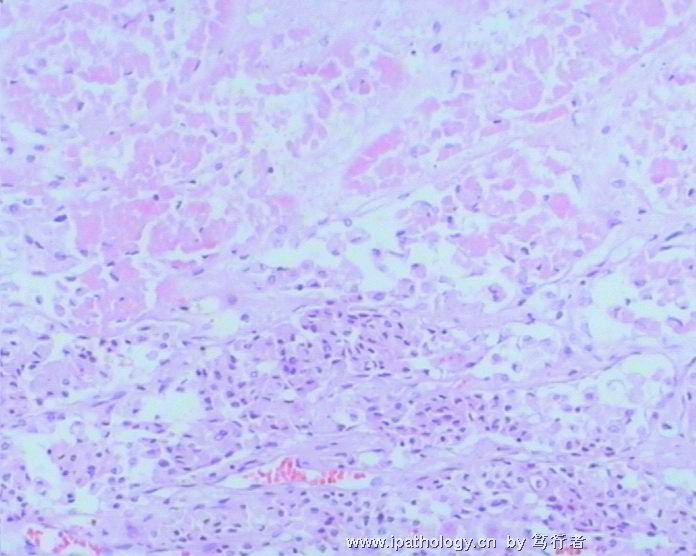
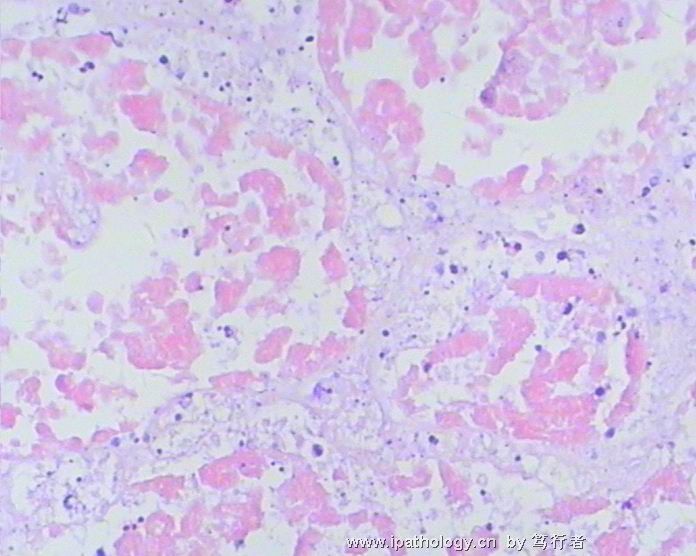
- 急切会诊--肾嗜酸细胞腺瘤能否恶变?
-
ZQH19811029 离线
- 帖子:458
- 粉蓝豆:1
- 经验:458
- 注册时间:2009-11-15
- 加关注 | 发消息
-
stevenshen 离线
- 帖子:343
- 粉蓝豆:2
- 经验:343
- 注册时间:2008-06-03
- 加关注 | 发消息
This is a real challenge case. I will try to give my thought about this case and hopefully it will be helpful. I look forward to hearing other opinions and final answers. It will be also helpful to know the tumor pathologic stage (fat or renal vein invasion) and metastasis Thanks.
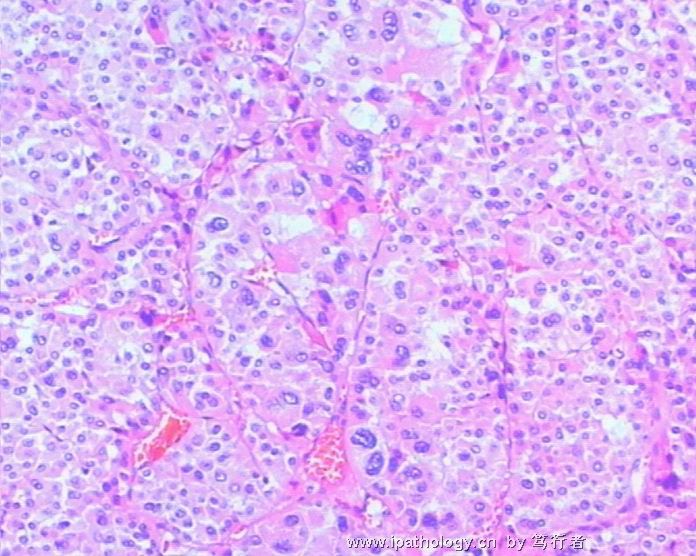
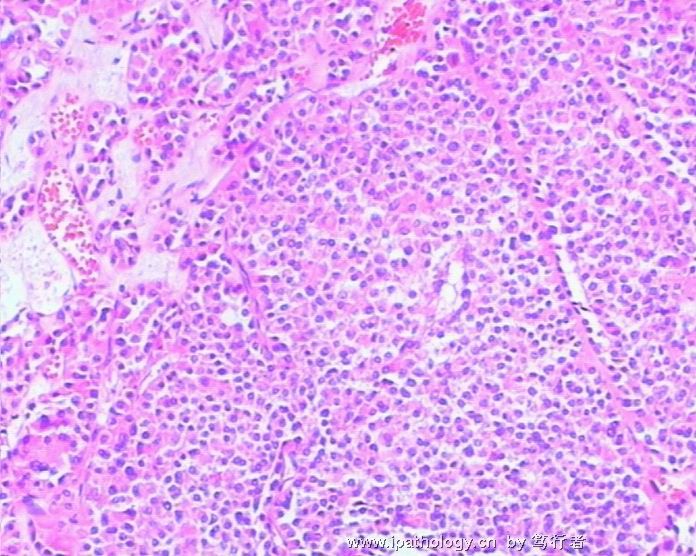
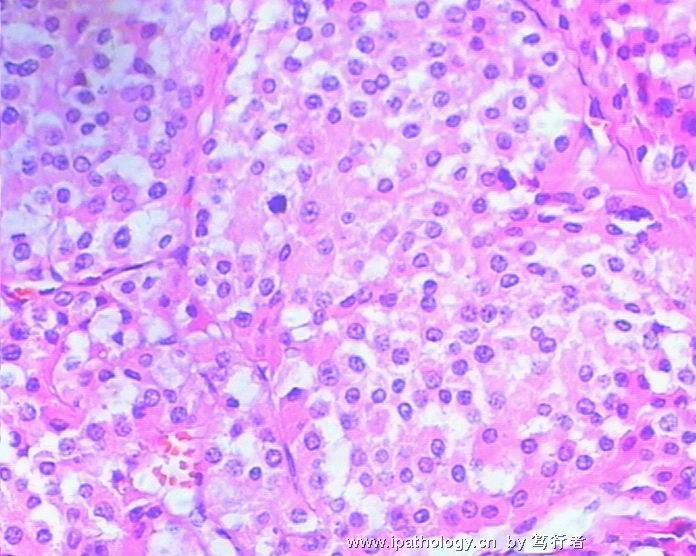
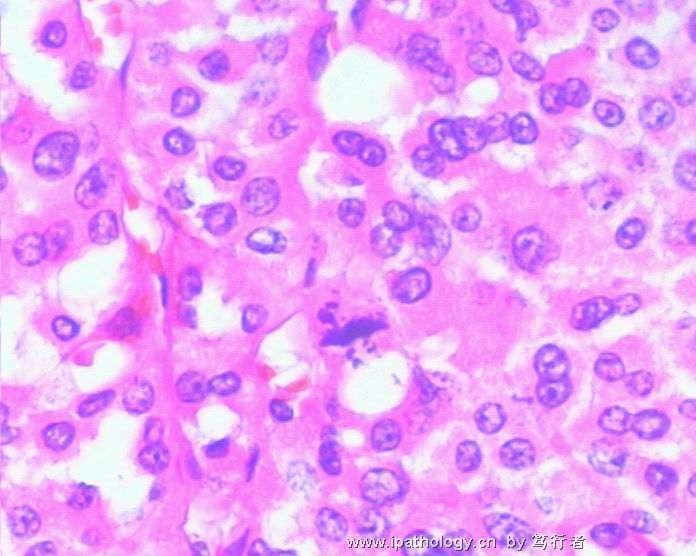
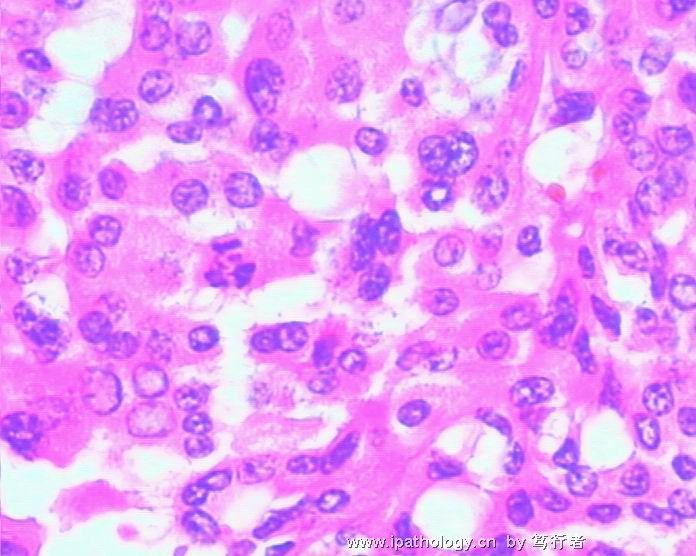
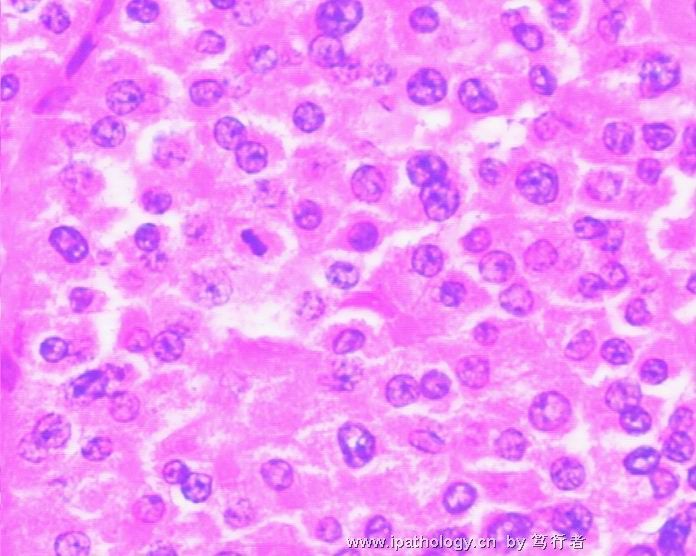
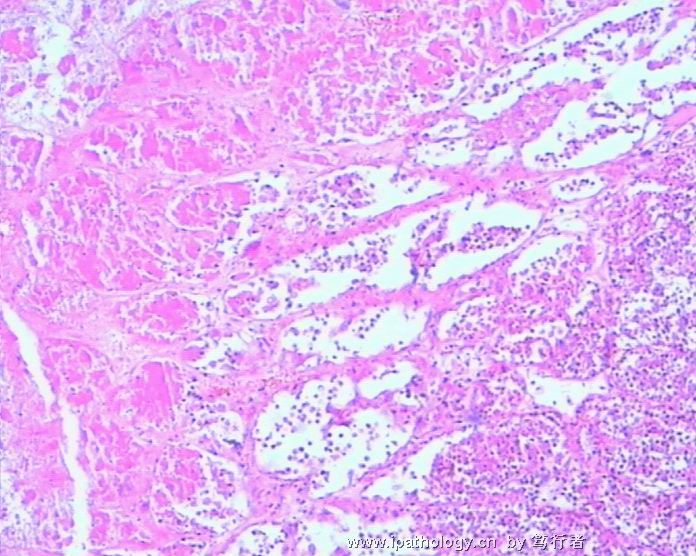
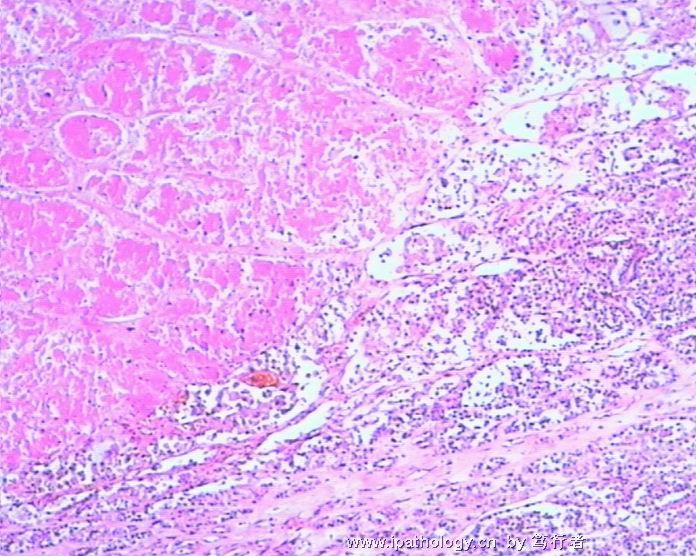
1、嗜酸细胞腺瘤?NO: There are certainly morphologic features of oncocytoma, but other features (focal papillary, true cytologic atypia and number of mitoses and atypical mitoses, necrosis and huge size all against diagnosis of oncocytoma. About 5% oncocytoma could have focal cytologic atypia or giant degenerating cells, but papillary and many mitoses, and tumor necrosis are not seen in a benign oncocytoma.
2、嫌色细胞癌嗜酸细胞亚型?Some people would agree with this diagnosis. I think it is not, again because of focal papillary and marked cytologic atypia and mitoses are not usually seen in eosinophilic type chromophobe RCC
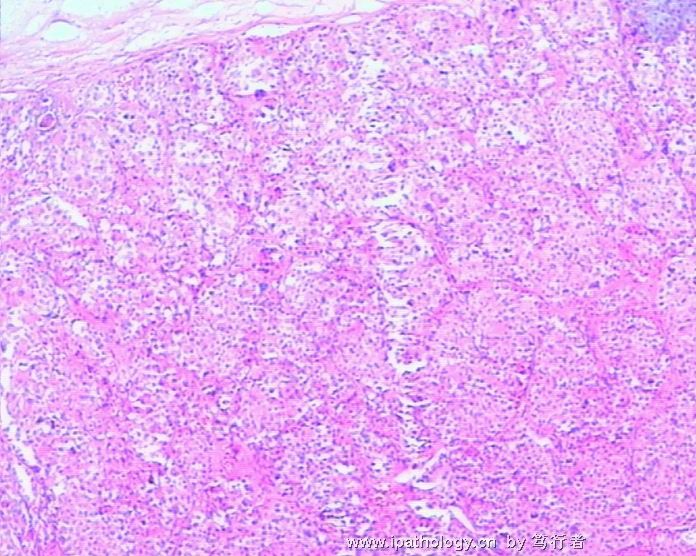
3、颗粒细胞型透明细胞癌?NO. The growth and vascular patterns are not that of a clear cell RCC with granular cells.
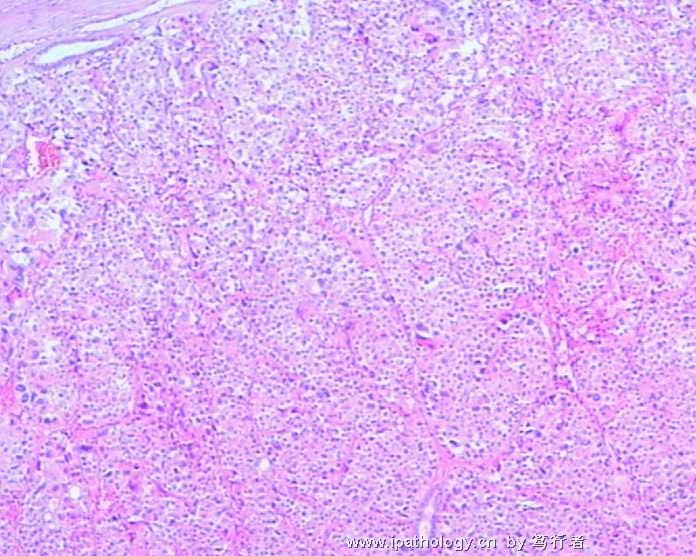
4、恶性嗜酸细胞腺瘤?NO. most people would not use this terminology anymore.
5. 还是腺瘤内有腺癌呢?This is a very interesting theory and it is certainly possible. It could be either transformation to a carcinoma (if we agree) from a oncocytoma or possibly a hybrid (mixed) oncocytom-chromophobe RCC.
6. I also think it is possible that it is a tubulopapillary RCC with eosinophilic cells.
7. For practical reason, the best diagnosis might be: unclassified RCC (oncocytic malignant RCC).
I don’t think immunostains will be particularly helpful because the heterogeneity of this tumor and overlapping staining profiles of most markers. Cytogenetic and chromosome analysis might be the only way to get a more definite diagnosis.
-
liguoxia71 离线
- 帖子:4174
- 粉蓝豆:3122
- 经验:4677
- 注册时间:2007-04-01
- 加关注 | 发消息
-
xieming1014 离线

- 帖子:116
- 粉蓝豆:2
- 经验:116
- 注册时间:2008-09-12
- 加关注 | 发消息
-
caotong_1978 离线

- 帖子:286
- 粉蓝豆:71
- 经验:698
- 注册时间:2006-12-13
- 加关注 | 发消息











